Religious Affiliation and Mental Health
Daniel K Judd
Daniel K. Judd, “Religious Affiliation and Mental Health,” inReligion, Mental Health, and the Latter-day Saints, ed. Daniel K. Judd (Provo, UT: Religious Studies Center, Brigham Young University, 1999), 245–280.
Daniel K Judd was assistant professor of ancient scripture at Brigham Young University when this was published. This article was originally published in AMCAP Journal 12:71–108; reprinted with permission.
Abstract
This chapter examines the possible relationships between religious affiliation, religiosity, and mental health. The study analyzes literature reviews comparing the mental health scores of members of several religious denominations. The general profiles for the Latter-day Saint, Roman Catholic, Protestant, Jewish, Hare Krishna, and nonreligious groups were within normal limits. Overall, these results contradict the suggestion that religiosity is facilitative of mental illness.
A renewed interest in the relationship between religiosity and mental health has developed. Bergin (1983) states that there is a “renascence of psychological interest occurring” (p. 170). Beit-Hallahmi (1973) states that in addition to a renewal of interest there exists an improvement in the quality of research. He further states, “After a golden age of theory and research on religion around the turn of the century, interest in this area had almost vanished from the social-science scene. The past decade has seen a renewal of interest and research on religion as a variable in social and private behavior. The increase has been not only in volume but also in quality” (p. v).
Great diversity in the operational and constitutive definitions of both religiosity and mental health exists. Strommen (1971) states: “For some [religiosity] means being affiliated with a religious institution and attending it regularly; for others religion is synonymous with expressed beliefs. . . . Some find their criteria of religiosity in religious acts; and others opt for mystical experiences. Some fail to recognize the multi-dimensionality of religion and assume they have tapped the essence when they have data on one dimension or on a subcategory within a dimension” (p. xvii).
Jahoda (1958) describes the ambiguity that exists in defining mental health, “There is hardly a term in current psychological thought as vague, evasive, and ambiguous as the term ‘mental health.’ That many people use it without even attempting to specify the idiosyncratic meaning the term has for them makes the situation worse, both for those who wish to promote mental health and for those who wish to introduce concern with mental health into systematic psychological theory and research” (p. 3).
While recognizing the difficulty in defining both variables, several theorists have attempted to do so. Hoult (1958) defines religion as “the belief in, and the attempt to relate favorably to (a) values thought to have some transcendental importance, and/
Jahoda (1958), commenting on the diverse definitions of mental health, has said, “Mental health as the opposite of mental disease is perhaps the most widespread and apparently simplest attempt at definition” (p. 10). While the defining of mental health as “the opposite of mental illness” is the definition most commonly used, Jahoda calls it an “unsuitable conceptualization” and outlines the following six aspects of a positive definition of mental health:
1. Accurate perception of reality which includes seeing what is really there in spite of pressures from the environment to distort;
2. Mastery of the situation which includes a sense of control and success in love, work, and play;
3. Autonomy which includes a sense of independence, self-determination, acceptance or rejection of influence, and the ability to surrender or commit oneself if one so desires;
4. Having a positive attitude towards oneself which includes acceptance, awareness, identity, and lack of self-consciousness;
5. Personal integration which includes an adequate balance of inner forces and a philosophy of life;
6. Self-actualization which includes a sense that one is growing and developing toward self-realization and long-range goals which one has set for himself. (Jahoda, cited in Maloney, 1983, p. 18)
Szasz has argued that neither a positive nor a negative definition of mental health is appropriate, as both are merely reflections of cultural values: what is defined as healthy in one culture may be defined as illness in another. As Szasz states, definition “entails . . . a covert comparison or matching of the patient’s ideas, concepts, or beliefs with those of the observer and the society in which they live” (Szasz as cited in Lowe, 1976, p. 56).
Review of Literature
Bergin (1983) and Lea (1982) each published literature reviews concerning religiosity and mental health through 1979 and 1977, respectively. Bergin’s review focused specifically on a meta-analysis of studies that dealt with at least one measure of religiosity correlated with at least one measure of mental pathology, such as the Minnesota Multiphasic Personality Inventory (MMPI) or the Manifest Anxiety Scale (MAS).
The impetus for Bergin (1983) was the widely held view among mental health professionals that religion is antithetical to mental health and rationality. Ellis is representative of this view: “Religiosity is in many respects equivalent to irrational thinking and emotional disturbance . . .. The elegant therapeutic solution to emotional problems is to be quite unreligious The less religious they are, the more emotionally healthy they will be” (as cited in Bergin, 1983, p. 170).
Bergin’s review of twenty-four studies (thirty outcomes) reports that the religiosity is facilitative of mental health in 4 of 9 MMPI measures, 1 of 3 neuroticism measures, 2 of 3 self-esteem measures, 1 of 4 for both hostility and inadequacy measures, 2 of 2 adjustment measures, and 1 of 1 measures of repression sensitization. Religiosity is negatively related to mental health in 5 of 10 anxiety measures, 1 of 3 self-esteem measures, and 1 of 1 measures of both ego strength and hostility.
No relationship between religiosity and mental health was reported in 5 of 10 measures of anxiety, 2 of 3 neuroticism measures, or 2 of 2 measures of irrational belief. There were five measures that showed significant positive statistical relationships and two that showed a significant negative relationship. (The term positive in this study represents religiosity being facilitative of mental health. The term negative represents religiosity as being facilitative of mental pathology.)
Hence, these findings do not support the assertion by Ellis that religiosity is “antithetical to emotional well being” (as cited in Bergin, 1983, p. 170), neither do the data provide more than “marginal support for the positive effect of religion,” for much of the data are contradictory (Bergin, 1983, p. 176).
Lea (1982) produced a literature review covering 1939–77. The reviewed studies investigated the relationship between religiosity and the variables of mental health as represented by social behavior.
Lea’s review of twenty-seven studies (thirty outcomes) suggests that religiosity has little or no effect upon the social health of the community and has a facilitative relationship with prejudice, excepting those individuals who score extremely high on measures of religiosity. Religiosity is conducive to feelings of personal inadequacy in students but not in the adult population. Students scoring high on religiosity measures were found to be more anxious and scored lower on measures of self-esteem than their less-religious counterparts. Religiosity is not significantly related to moral behavior or social deviancy. Adjusting the outcomes to reflect the positive (facilitative), negative (antithetical), or neutral relationship of religiosity and mental health, of the twenty-eight outcomes reviewed, 44 percent suggest a negative relationship, 41 percent a positive relationship, and 15 percent a neutral relationship. While Lea (1982) reports “the data describe a potential positive relationship between religion and psychological health” (p. 340), he also writes of the importance of caution in interpreting the data: “Methodological problems relating to defining ‘religion’ and ‘mental health’ and to correlational data require caution in interpretation Limitations exist in the number and type of studies conducted, their methodology, and the difficulty in interpreting their results” (p. 347).
Affiliation as a Measure of Religiosity
While Bergin (1983) and Lea (1982) have published literature reviews covering a period from 1939 through 1979, their reviews, by their own design, have not been comprehensive. Lea totally omitted the operational definitions of religiosity while Bergin included such definitions in fourteen of twenty-four studies. I have expanded both the Bergin and Lea studies to include the specific measures of religiosity and mental health. Furthermore, this forthcoming article will review the research that has been published since the reviews of Bergin and Lea. (See end of book Appendix for a summary of this article.) Inasmuch as my other article will address the general concerns of religiosity and mental health, it is intended that the remainder of this paper focus on the affiliation dimension of religiosity and its relationship to mental health. Lea (1982) suggests that “little research exists on the relationship between specific denominations and mental health” (p. 336). Consequently, the sampling of specific religious denominations is suggested as an area for further research.
By examining the empirical evidence derived from religious affiliation, I intend to identify what influence this variable may have upon the relationship of religiosity and mental health.
Table 13.1 contains studies concerning the relationship of religious affiliation and mental health from 1939 through March 1985. Of the twenty-two studies reported in Table 13.1, seven indicated a comparison between Catholic, Protestant, and Jewish religions while eight made a comparison between religious affiliates (no specific denominations mentioned) and nonaffiliates. Two studies compared Catholicism and specific Protestant religions such as the Baptist, Methodist, Lutheran, and Episcopalian. Two studies focused on the Unification Church and one study respectively on the Jehovah’s Witnesses, Hare Krishna, Christian Science, and Baha’i.
The data indicate little support for the assertion that religiosity is facilitative of psychopathology. Of the eleven studies reporting a comparison of nonreligious and religious samples, three report the religious sample being less “mentally healthy,” four report the religious sample having greater “mental health,” and four report equal “mental health.”
Concerning denominational comparisons, the data indicate that Catholics, Protestants, and Jews are equal with regard to prejudice, MMPI scores, psychological competence, marital stability, and humanitarianism/ egalitarianism.
Protestants abuse alcohol less frequently than Catholics and Jews. Jehovah’s Witnesses are treated more frequently for schizophrenia than are people from other religions. Catholics and Baptists are hospitalized in mental institutions more frequently than Methodists or Lutherans.
The data indicate a preponderance of research concerning affiliated vs. nonaffiliated and Catholic vs. Protestant comparisons. Capps (1984) (journal editor for The Scientific Study of Religion) states his perception of the present situation: “Since I began receiving manuscripts in June 1982, there have been some 53 submissions . . . on a specific religious denomination or aspect thereof. . . . There were twelve denominations represented, with the following breakdown: Catholic, 17; Judaism, 11; Mormon, 9; Mennonite, 4; Seventh-day Adventists, 4; Episcopal, 2; and one each for Assembly of God, Baptist, Jehovah’s Witness, Lutheran, Pentecostal, and Quaker” (p. 108). While Capps continues and calls for studies concerning “various churches within mainline protestantism” (p. 108), it is my perception that much can be done with the existing studies in making meaningful comparisons.
Method
Studies were selected from the review of literature which reported the following: (a) specific religious affiliation and (b) scores from the MMPI. The studies fitting these criteria were Ross (1983), Bohrnstedt, Borgatta, and Evans (1968), Groesch and Davis (1977), and Panton (1979). The latter two studies were excluded, for they dealt with extreme populations—psychiatric patients and prison inmates, respectively. The sample consisted of 816 Catholic, 1,953 Protestant, 695 Jewish, 203 nonreligious college students, and 42 Hare ICrishna devotees. Also, previously unreported MMPI data were obtained from 2,751 members of The Church of Jesus Christ of Latter-day Saints (student sample data obtained from Burton Kelly). In addition to the extracting of data from previous studies, I contacted and administered the MMPI to local groups of Hare Krishna, Baha’i, and Seventh-day Adventists. Due to the small sample sizes available, these data are not included in this analysis.
MMPI mean scores for the three validity scales and each of the ten clinical scales were extracted and compared for each of the three data bases. The authors of the various studies consulted did not include standard deviation data for their respective samples. However, inasmuch as this report is the first to include LDS data, standard deviation scores for this sample were reviewed and found to be consistent with a normal population. Visual summaries and descriptive statistics representing the MMPI mean scores and T-scores are created for comparative clarity.
Results
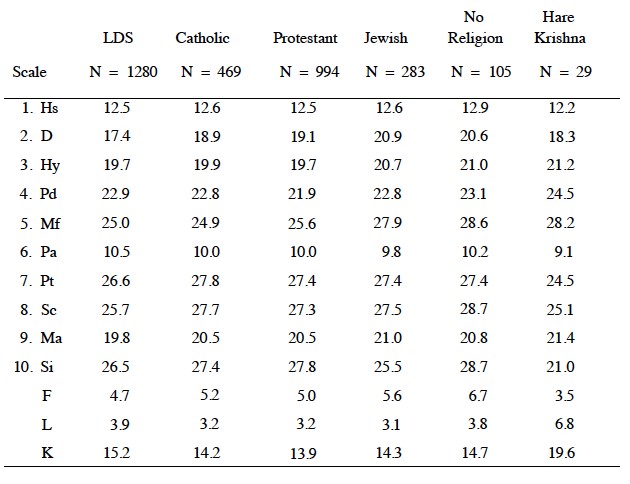
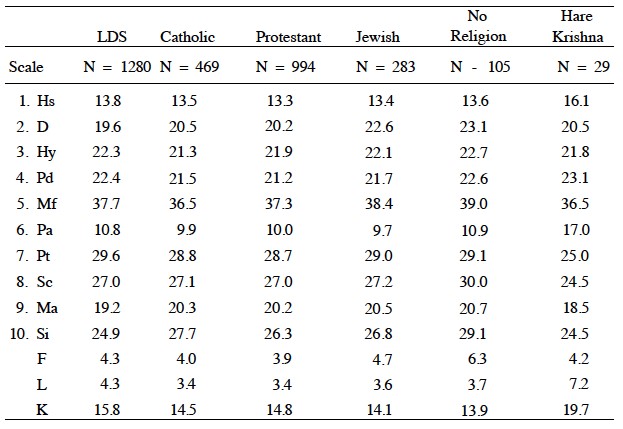
Tables 13.2 (male) and 13.3 (female) contain the mean scores for each of the specific denominations surveyed. Since the MMPI is normalized separately for males and females, respective summaries are reported.
Table 13.2: Mean MMPI Scores for Respective Religious Affiliations (MALE) (Scores corrected for K)
MMPI Interpretations
Duckworth (1979) has developed the MMPI Interpretation Manual for Counselors and Clinicians in which she has made an exhaustive review of research concerning the MMPI. This research has been utilized by the author in offering interpretations of the MMPI profiles created for each of the groups being studied. For a definition of the MMPI scales, see Appendix B.
Table 13.3: Mean MMPI Scores for Respective Religious Affiliations (FEMALE) (Scores corrected for K)
LDS MMPI Profiles
The scores obtained from the LDS sample were generally typical of the majority of “normal” people taking the MMPI. Both male and female LDS subjects were willing to admit to general human faults—their scores did not indicate any evidence of attempting to “fake good.” Individuals with scores similar to the LDS sample seldom show evidence of mental pathology. Catholic MMPI Profiles
The scores obtained from the Catholic sample were within normal limits. Male and female profiles indicated that they are willing to admit to general human faults. No indication of mental pathology was observed.
Protestant MMPI Profiles
Scores from the Protestant sample were within normal limits. Protestant females appeared to be “nonworriers,” secure with them selves. They may appear to some as being “non-task oriented” (Duckworth, 1979, p. 149).
Jewish MMPI Profiles
The scores obtained from the Jewish sample were within normal limits on all scales. Jewish males appeared to be interested in aesthetics and to be somewhat passive. Jewish female profiles indicated the desire for traditional female roles.
Nonreligious MMPI Profiles
Scores obtained from those who did not indicate a preference for religious affiliation were within the normal limits for all scales measured.
Males and females in this category may think differently than other people. Duckworth (1979) states that people scoring similar to this profile may be “avant-garde [different] or highly creative people” (p. 164). People with profiles similar to this often indicate a concern with social problems. Duckworth further states: “With college educated persons, this level usually indicates concern about the social problems of the world Other people with this elevation may have a situational crisis such as marital discord. In this latter instance, the elevation tends to go down after the problem is resolved” (p. 177).
Hare Krishna MMPI Profiles
The scores obtained from the Hare Krishna were within normal limits on all of the scales excepting scale 6 (paranoia). Hare Krishna females’ scores indicated that they were interpersonally sensitive to what others thought of them. Duckworth (1979) states: “In addition to sensitivity . . . suspiciousness is usually present. The client may assume that other people are after him or her. Righteous indignation also is usually present” (p. 139). Hare Krishna female profiles indicated they may not be interested in being considered feminine, although this may be an indication of cultural differences. Hare Krishna males and females presented themselves as being virtuous, conforming, and self-controlled. The scores of Hare Krishna men indicated they were generally poised and confident in social and group situations but typically not satisfied with the social condition of the world and would like change.
Discussion
This study represents an analysis of 6,270 subjects affiliated among five different religions. From the thirteen different measures of mental health for each of these five religions studied (sixty-five measures), only one scale on one sample was outside the normal limits on the MMPI. These data contradict the notion set forth by Albert Ellis that religiosity is facilitative of mental illness (as cited in Bergin, 1983).
While there are differences in the interpretations of the MMPI profiles for the five religions studied, they were all quite similar and indicated no extreme difference as to the presence or absence of mental pathology.
Inasmuch as this study has operationally defined religion in terms of religious affiliation, I hope that future research will examine the relationship of the MMPI and other dimensions of religiosity. Also, because thirteen research scales have been added to the traditional MMPI, I feel that these scales should be reported in future studies.
Appendix A
Judd (1985) reviewed 167 studies concerning the relationship of religiosity and mental health. These studies covered the years 1928 to 1985. The findings revealed little support for the assertion that religiosity is antithetical to mental health. High levels of specific religiosity measure were reported as being facilitative of marital and family stability, personal adjustment, and well-being. Religiosity was reported to have curvilinear relationship with prejudice, ethnocentrism, and authoritarianism.
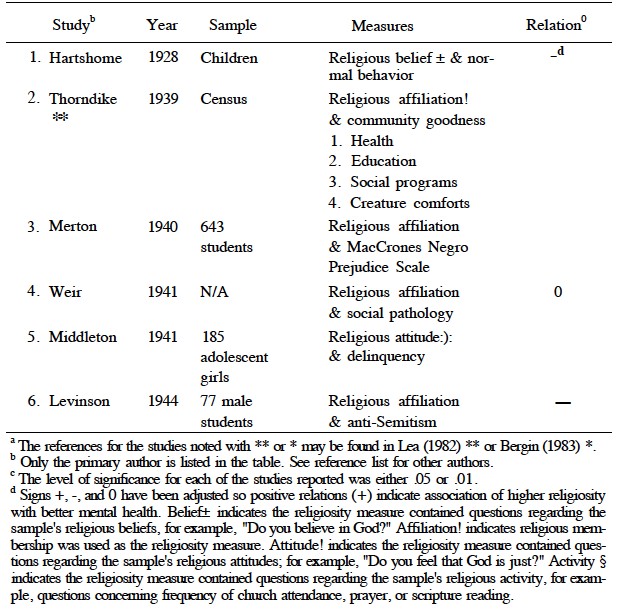
Table 13.4 lists the year, type of sample, measures, and outcome for each of the studies reviewed.
Table 13.4: A Comprehensive & Contemporary Review of Literature Concerning Religiosity and Mental Health 1928–85 Including Lea ** (1982) and Bergin * (1983) Reviewsa)
Appendix B
The Minnesota Mutliphasic Personality Inventory
The Minnesota Multiphasic Personality Inventory is a true/
Since its initial publication, several attempts have been made to modify the 566 question format. While various short forms have been proposed, few revisions have proved as satisfactory as the original format.
Validity Scale
L Scale. Fifteen items all scored in the false direction and often associated with an attempt to make a good impression.
F Scale. Sixty-four items involving a broad spectrum of psychopathology and often associated with an attempt to fake mental symptoms.
K Scale. Thirty items generally reflecting defensiveness or guardedness.
Clinical Scales
I.Hypochondriasis (Hs). Thirty-three items expressing concern regarding bodily functions.
2. Depression (D). Sixty items expressing moodiness, dysphoria, or hopelessness.
3.Hysteria (Hy). Sixty items revealing those who may respond to stress by use of conversion symptomology.
4. Psychopathic Deviate (Pd). Fifty items generally identifying antisocial behavior tendencies.
5. Masculinity/
6. Paranoia (Pa). Forty items generally eliciting delusional material reflecting feelings of grandeur or persecution.
7. Psychasthenia (Pt). Forty-eight items identifying excessive sensitivity, doubt, or indecision.
8. Schizophrenia (Sc). Seventy-eight items reflecting unusual thought processes or personal perception.
9. Hypomania (Ma). Forty-six items identifying impulses toward increased inability, nonproductive activity, and mood difficulties.
10. Social Introversion (Si). Seventy items reflecting self-concept difficulties and a tendency to withdraw.
References
Alexander, J. E., & Adelstein, A. M. (1960). Studies in the psychology of death. In H. P. David & J. C. Brengleman (Eds.), Perspectives in personality research (pp. 65–92). New York: Springer.
Allen, R. O. (1965). Religion and prejudice: An attempt to clarify the patterns of relationship. Dissertation Abstracts, 26, 1A1\.
Allen, R. O., & Spilka, B. (1967). Committed and consensual religion: A specification of religion prejudice relationships. Journal for the Scientific Study of Religion, 6, 191–206.
Allport, G. W. (1954). The nature of prejudice. Cambridge: Addison-Wesley.
Allport, G. W., & Kramer, B. J. (1946). Some roots of prejudice. Journal of Psychology, 22, 9–39.
Angell, R. C. (1951). The moral integration of American cities. American Journal of Sociology, 57.
Armstrong, R. C, Larsen, G. L., & Mourer, S. A. (1962). Religious attitudes and emotional adjustment. Journal of Psychological Studies, 13, 35–47.
Babchuk, N., Crockett, H. J., & Ballweg, J. A. (1967). Change in religious affiliation and family stability. Social Forces, 45, 551–555.
Bagley, C. (1970). Relation of religion and racial prejudice in Europe. Journal for the Scientific Study of Religion, 9, 219–225.
Bateman, M. M., & Jensen, J. S. (1958). The effect of religious background on modes of handling anger. Journal of Social Psychology, 47, 133–141.
Beit-Hallahmi, B. (Ed.). (1973). Research in religious behavior: Selected readings. Monterey: Brooks/
Bergin, A. E. (1983). Religiosity and mental health: A critical reevaluation and meta-analysis. Professional Psychology: Research and Practice, 14 (2), 170–183.
Bergin, A. E., Masters, K. S., & Richards, P. S. (1987). Religiousness and mental health reconsidered: A study of an intrinsically religious sample. Journal of Counseling Psychology, 34(2), 197–204.
Bettleheim, B., & Janowitz, M. (1950). Dynamics of prejudice. New York: Harper.
Blumm, S. B., & Mann, J. H. (1960). The effect of religious membership on religious prejudice. Journal of Social Psychology, 52, 97–101.
Bohrnstedt, G. W., Borgatta, E. R, & Evans, R. R. (1968). Religious affiliation, religiosity, and MMPI scores. Journal for the Scientific Study of Religion, 7, 255–258.
Brannon, R. (1970). Gimme that old-time racism. Psychology Today, 3(11), 42–44.
Burgess, J. H., & Wagner, R. L. (1971). Religion as a factor in extrusion to public mental hospitals. Journal for the Scientific Study of Religion, 10, 23 7–240.
Campbell, A. (1971) White attitudes toward black people. Ann Arbor: Institute for Social Research, University of Michigan.
Capps, D. (1984). From the editor. Journal for the Scientific Study of Religion, 23 (2), 108.
Chalfant, P. H. (1983). Religious affiliation, religiosity, and racial prejudice: Anew look at old relationships. Review of Religious Research, 48 (2), 155–161.
Conway, R, & Siegelman, J. (1982). Have cults created a new mental illness? Review of Religious Research, 48(2), 155–161.
Duckworth, J. (1979). MMPI interpretation manual for counselors and clinicians. Muncie, IN: Accelerated Development.
Durkheim, E. (1954). The elementary forms of religious life (J. W. Swain, Trans.). Glencoe, IL: Free Press.
Ebaugh, H. R., Richman, K., & Chafetz, J. S. (1984). Live crises among the religiously committed: Do sectarian differences matter? Journal for the Scientific Study of Religion, 23 (1), 19–31.
Eisenman, R., & Cole, S. N. (1964). Prejudice and conservatism in denominational college students. Psychological Reports, 14, 644.
Ellis, A. (1980). Psychotherapy and atheistic values: A response to A. E. Bergin’s “Psychotherapy and religious values.” Journal of Consulting and Clinical Psychology, 48 (5), 635–639.
Evans, R. I. (1952). Personal values as factors in anti-Semitism. Journal of Abnormal and Social Psychology, 47, 749–756.
Feagin, J. R. (1964). Prejudice and religious types: A focused study of southern fundamentalists. Journal for the Scientific Study of Religion, 4, 3–13.
Feifel, H. (1974). Religious conviction and fear of death among the healthy and terminally ill. Journal for the Scientific Study of Religion, 13, 353–360.
Fislinger, E. E., & Wilson, M. E. (1984). Religiosity, socioeconomic rewards, and family development: Predicators of marital adjustment. Journal of Marriage and the Family, 46, 663–670.
Frenkel-Brunswik, E., & Sanford, R. N. (1945). Some personality factors in anti- Semitism. Journal of Psychology, 20, 271–291.
Freud, S. (1953). The future of an illusion (W. D. Robinson, Trans.). New York: Doubleday.
Funk, R. A. (1955). A survey of religious attitudes and manifest anxiety in a college population. Dissertation Abstracts, 15, 2569.
Galanter, M. (1980). Psychological induction into the large group: Findings from a modern religious sect. American Journal of Psychiatry, 137 (12), 1574–1579.
Galanter, M. (1982). Charismatic sects and psychiatry: An overview. American Journal of Psychiatry, 139 (12), 1539–1548.
Galanter, M., Buckley, P., & Deutsch, A. (1980). Large group influence for decreased drug use: Findings from two contemporary religious sects. American Journal of Alcohol and Drug Abuse, 7, 291–304.
Galanter, M., Rabkin, R., & Rabkin, J. (1979). The “Moonies”: A psychological study of conversion and membership in a contemporary religious sect. American Journal of Psychiatry, 136, 165–170.
Glenn, N. D. (1982). Interreligious marriage in the United States: Patterns and recent trends. Journal of Marriage and Family, 44 (3), 555–566.
Glenn, N. D., & Weaver, C. N. (1978). A multivariate, multisurvey study of marital happiness. Journal of Marriage and the Family, 40, 269–282.
Glock, C. Y, & Stark, R. (1965). Religion and society in tension. Chicago: Rand McNally.
Glock, C. Y, & Stark, R. (1966). Christian beliefs and anti-Semitism. New York: Harper & Row.
Gorsuch, R. L., & Aleshire, D. (1974). Christian faith and ethnic prejudice: Areview and interpretation of research. Journal for the Scientific Study of Religion, 13, 281–307.
Gorsuch, R. L., & McFarland, S. (1972). Single vs. multiple item scales for measuring religious values. Journal for the Scientific Study of Religion, 11, 53–64.
Gough, H. G. (1951). Studies of social intolerance: IV. Related social attitudes. Journal of Social Psychology, 33, 263–269.
Gray, D. B., & Revelle, W. (1974). A multidimensional religious attitude inventory related to multiple measures of race. Journal of Social Psychology, 92, 153–154.
Gregory, W. E. (1957). The orthodoxy of the authoritarian personality. Journal of Social Psychology, 45, 217–232.
Groesch, S. J., & Davis, W. E. (1977). Psychiatric patients’ religion and MMPI responses. Journal of Clinical Psychology, 33(1), 168–171.
Gurin, G, Veroff, J., & Feld, S. (1975). Americans view their mental health. Ann Arbor: Social Science Archive Institute for Social Research.
Hadaway, C. K. (1978). Life satisfaction and religion: Areanalysis. Social Forces, 57 (2), 636–643.
Hadaway, C. K., Elifson, K. W., & Peterson, D. M. (1984). Religious involvement and drug use among urban adolescents. Journal for the Scientific Study of Religion, 23 (2), 109–128.
Hardin, J., Kutner, B., & Proshansky, H. (1954). Prejudice and ethnic relations. In G. Lindzey (Ed.), Handbook of social psychology. Reading, MA: Addison- Wesley.
Hartshorne, H., & May, M. A. (1928). Studies in the nature of character: I. Studies in deceit. New York: MacMillan.
Hathaway, S. R. & McKinley, J. C. (1943). Manual for the Minnesota Multiphasic Personality Inventory. Minneapolis: University of Minnesota Press.
Heaton, T. B. (1984). Religious homogamy and marital satisfaction reconsidered. Journal of Marriage and the Family, 46 (3), 729–733.
Hoge, D., & Carroll, J. W. (1973). Religiosity and prejudice in northern and southern churches. Journal for the Scientific Study of Religion, 12, 181–197.
Hood, R. W., Jr. (1974). Psychological strength and the report of intense religious experience. Journal for the Scientific Study of Religion, 13, 65–71.
Hoult, T. F. (1958). The sociology of religion. New York: Holt, Rinehart & Winston.
Humanist manifesto I & II. (1973). Buffalo: Prometheus Books.
Hunt, R. A., & King, M. B. (1978). Religiosity and marriage. Journal for the Scientific Study of Religion, 17, 399–406.
Jahoda, M. (1958). Current concepts of positive mental health. New York: Basic Books.
James, W. (1902). The varieties of religious experience. New York: Longmans.
Johnson, M. A. (1974). The relationship of religious commitment to self-esteem. Unpublished master’s thesis, Brigham Young University, Provo, UT.
Jones, M. B. (1958). Religious values and authoritarian tendency. Journal of Social Psychology, 48, 83–87.
Judd, D. K. (1985). Religiosity and mental health: A literature review, 1928–1985. Unpublished master’s thesis, Brigham Young University, Provo, UT.
Keedy, T. C. (1958). Anomie and religious orthodoxy. Sociology and Social Research, 43, 34–37.
Kelly, J., Ferson, J., & Holtzman, W. (1958). The measurement of attitudes towards the negro in the South. Journal of Psychology, 48, 305–317.
Kersten, L, K. (1970). The Lutheran ethic: The impact of religion on laymen and clergy. Detroit: Wayne State University Press.
Kilbourne, B. K. (1983). The Conway and Seigelman claims against religious cults: An assessment of their data. Journal for the Scientific Study of Religion, 22 (4), 380–385.
King, M. D., & Hunt, R. A. (1972). Measuring religious dimensions. Dallas: Congregational Involvement Study.
Kirkpatrick, C. (1949). Religion and humanitarianism: A study of institutional implications. Psychological Monographs, 63 (304).
Kunz, P. R., & Albrecht, S. L. (1977). Religion, marital happiness, and divorce. International Journal of Sociology of the Family, 7, 227–232.
Lantz, H. (1949). Religious participation and social orientation of 1,000 university students. Journal of Sociological Social Research, 33, 285–290.
Lea, G. (1982). Religion, mental health, and clinical issues. Journal of Religion and Health, 21 (4), 336–351.
Levinson, D. J., & Sanford, R. N. (1944). A scale for the measurement of anti- Semitism. Journal of Psychology, 17, 339–370.
Lindenthal, J. L., Myers, J. K., Pepper, M. P., & Stern, M. S. (1970). Mental stature and religious behavior. Journal for the Scientific Study of Religion, 9, 143–149.
Lowe, C. M. (1976). Value orientations in counseling and psychotherapy: The meanings of mental health (2nd ed.). Cranston, RI: Carroll.
McDonald, C. B., & Luckett, J. B. (1983). Religious affiliation and psychiatric diagnoses. Journal for the Scientific Study of Religion, 22 (1), 15–37.
McGrath, J. E. (1961). Religious group differences in value orientations, interpersonal perceptions and personal adjustment. Paper presented at the meeting of the Society for the Scientific Study of Religion, Cambridge, MA.
Maddox, G. L. (1964). High school student drinking behavior: Incidental information from two national surveys. Quarterly Journal of the Studies on Alcohol, 25, 339^347.
Maloney, H. N. (Ed.). (1983). Wholeness and holiness. Grand Rapids: Baker.
Martin, C, & Nichols, R. C. (1962). Personality and religious belief. Journal of Social Psychology, 56, 3–8.
Merton, R. K. (1940). Facts and factiousness in ethnic opinionnaires. American Sociological Review, 5, 13–28.
Middleton, R. (1973). Do Christian beliefs cause anti-Semitism? American Sociological Review, 38, 33–52.
Middleton, W. C, & Fay, P. J. (1941). Attitudes of delinquent and non-delinquent girls toward Sunday observance, the Bible, and war. Journal of Educational Psychology, 32, 555–558.
Mobert, D. O., & Taves, M. J. (1965). Church participation and adjustment in old age. In A. M. Rose & W. A. Peterson (Eds.), Older people and their social world. Philadelphia: F. A. Davis.
Ness, R. C, & Wintrob, R. M. (1980). The emotional impact of fundamentalist religious participation: An empirical study of intragroup variation. American Journal of Orthopsychiatry, 50 (2), 302–315.
Nias, D. K. B. (1972). The structuring of social attitudes in children. Child Development, 43,211–219.
Obenhaus, V., & Schroeder, W. W. (1963). Church affiliations and attitudes toward selected public questions in a typical midwest county. Rural Sociology, 28, 35–47.
O’Neil, W. M., & Levinson, D. J. (1953). A factorial exploration of authoritarianism and some of its ideological concomitants. Journal of Personality, 22, 449–463.
O’Reilly, C. T. (1958). Noninstitutionalized religion and happiness. Journal of Sociological Research, 42, 119–121.
O’Reilly, C. T., & O’Reilly, E. J. (1954). Religious beliefs of Catholic college students and their attitude toward minorities. Journal of Abnormal and Social Psychology, 49, 378–380.
Panton, J. H. (1979). An MMPI item content scale to measure religious identification within a state prison population. Journal of Clinical Psychology, 35 (3), 588–591.
Pargament, K. I., Tyler, F. B., & Steele, R. E. (1979). Is fit it? The relationship between church/
Parker, J. H. (1968). The interaction of negroes and whites in an integrated church setting. Social Forces, 46 (3), 359–366.
Parry, H. J. (1949). Protestants, Catholics and prejudice. International Journal for Opinions and Attitude Research, 3, 205–213.
Pattison, E. M., & Pattison, M. L. (1980). “Ex-gays”: Religiously meditated change in homosexuals. American Journal of Psychiatry, 737(12), 1153—1162.
Perkins, H. W. (1985). A research note on religiosity as opiate or prophetic stimulant among students in England and United States. Review of Religious Research, 26 (3), 269–280.
Pettigrew, T. F. (1959). Regional differences in anti-negro prejudice. Journal of Abnormal and Social Psychology, 59, 28–36.
Porterfield, A. L. (1946). Religious affiliation. Journal of Social Research, 31, 23–219.
Prothro, E. T., & Jensen, J. A. (1950). Interrelations of religious and ethnic attitudes in selected southern populations. Journal of Social Psychology, 32,45–49.
Putney, S., & Middleton, R. (1961). Religion and authoritarianism. Social Forces, 39, 285–290.
Pyron, B. (1961). Belief, Q-sort, Allport-Vernon study of values and religion. Psychological Reports, 8, 399–400.
Ragan, R. L. (1963). Attitudes of white Methodist church members in selected Los Angeles metropolitan area churches toward residential segregation of the negro. Dissertation Abstracts, 24, 2615.
Ranck, J. G. (1955). Some personality correlates of religious attitude and belief. Dissertation Abstracts, 15, 878–879.
Rokeach, M. (1960). The open and closed mind. New York: Basic Books.
Rokeach, M. (1969). Religious values and social compassion. Review of Religious Research, 11, 3–23.
Rosenblith, J. F. (1949). Areplication of “some roots of prejudice. “Journal of Abnormal and Social Psychology, 44, 470–489.
Rosenblith, J. F. (1957). How much invariance is there in the relations of “prejudice scores” to experiential and attitudinal variables? Psychological Reports, 3, 217–241.
Rosenblum, A. L. (1958). Ethnic prejudice as related to social class and religiosity. Sociological Social Research, 43, 272–275. Ross, M. G. (1950). Religious beliefs of youth. New York: Association Press.
Ross, M. W. (1983). Clinical profiles of Hare Krishna devotees. American Journal of Psychiatry, 104 (4), 416–420.
Sanai, M. (1952). An empirical study of political, religious, and social attitudes. British Journal of Psychiatry, 5, 81–92.
Sanford, R. N. (1950). Ethnocentrism in relation to some religious attitudes and practices. In T. W. Adorno (Ed.), The authoritarian personality. New York: Harper.
Sanford, R. N., & Levinson, D. J. (1948). Ethnocentrism in relation to some religious attitudes and practices. American Psychologist, 3, 350–351.
Sanua, V. D. (1969). Religion, mental health, and personality: Areview of empirical studies. American Journal of Psychiatry, 125(90), 1203–1213.
Schlegel, R. P., & Crawford, C. A. (1978). Multidimensional locus of control and drug use among high school students. Canadian Journal of Behavioral Science, 10, 141–151.
Schofield, W. (1959). Religion and schizophrenia. Journal of Abnormal Social Psychology, 59, 216–225.
Scholl, M. E., & Becker, J. (1964). A comparison of the religious beliefs of delinquent and non-delinquent Protestant adolescent boys. Religious Education, 59, 250–253.
Schumm, W. R., Bollman, S. R., & Jurich, A. P. (1982). The “marital conventionalization” argument: Implications for the study of religiosity and marital satisfaction. Journal of Psychology and Theology, 10 (3), 236–241.
Shaver, P., Lenauer, M., & Sadd, S. (1980). Religiousness, conversion, and subjective well-being: The “healthy-minded” religion of modern American women. American Journal oj’Psychiatry, 137(12), 1563–1568.
Shinert, G, & Ford, C. E. (1958). The relation of ethnocentric attitudes to intensity of religious practice. Journal of Educational Sociology, 32, 157–162.
Shrum, W. (1980). Religion and marital instability: Change in the 1970s? Review of Religious Research, 21 (2), 135–147.
Siegman, A. W. (1962). A cross-cultural investigation of the relationship between religiosity, ethnic prejudice and authoritarianism. Psychological Reports, 11, AX9-A2A.
Skinner, B. F. (1948). Walden two. New York: Macmillan.
Smith, R M. (1949). Organized religion and criminal behavior. Sociological Social Research, 33, 363–367.
Smith, R M. (1956). Prisoners ‘attitudes toward organized religion. Religious Education, 51, 462–464.
Spencer, J. (1975). The mental health of Jehovah’s Witnesses. British Journal of Psychiatry, 126, 556–559.
Spendlove, D. C, West, D. W., & Stanish, W. M. (1984). Risk factors and the prevalence of depression in Mormon women. Social Science and Medicine, 18 (6), 491–495.
Spilka, B. (1958). Religious attendance and prejudice. New York University—Psychological Newsletters.
St. George, A., & McNamara, P. H. (1984). Religion, race and psychological wellbeing. Journal for the Scientific Study of Religion, 23, 351–363.
Stack, S. (1983). The effect of the decline in institutionalized religion on suicide, 1954–1978. Journal for the Scientific Study of Religion, 22 (3), 239–252.
Strickland, B. R., & Weddell, S. C. (1972). Religious orientation, racial prejudice, and dogmatism: A study of Baptists and Unitarians. Journal for the Scientific Study of Religion, 11, 395–399.
Strommen,M. P. (1967). Religious education and the problem of prejudice. Religious Education, 62, 52–59.
Strommen, M. P. (1971). Research on religious development: A comprehensive handbook. New York: Hawthorne.
Strommen, M. P. (1972). A study of generations. Minneapolis: Augsburg.
Struening, E. L. (1963). Anti-democratic attitudes in midwest university. In H. H. Remmers (Ed.), Anti-democratic attitudes in American schools. Evanston, IL: Northwestern University Press.
Strunk, 0. (1959). Interest and personality patterns of preministerial students. Psychological Reports, 5, 740.
Tate, E. D., & Miller, G. R. (1971). Differences in value systems of persons with varying religious orientations. Journal for the Scientific Study of Religion, 10, 357–365.
Thorndike, E. L. (1939). American cities and states. American New York Academy of Sciences, 39, 213–298.
Turbeville, C, & Hyde, R. E. (1946). A selected sample of attitudes of Louisiana State University towards the negro: A study in public opinion. Social Forces, 24, 447^150.
Watson, P. J., Hood, R. W., Jr., & Morris, R. J. (1984). Religious orientation, humanistic values, and narcissism. Review of Religious Research, 25 (3).
Weir, E. (1941). Criminology: A scientific study. Joliet, IL: Institute for the Scientific Study of Crime.
Whitam, F. L. (1962). Subdimensions of religiosity and race prejudice. Review of Religious Research, 3, 166–174.
Wilkinson, M. L., & Tanner, W. C. (1980). The influence of family size, interaction, and religiosity on family affection in a Mormon sample. See chapter 6 in this volume.
Williams, R. M., Jr. (1964). Strangers next door. Englewood Cliffs, NJ: Prentice- Hall.
Wilson, W. C. (1960). Extrinsic religious values and prejudice. Journal of Abnormal and Social Psychology, 60, 286–288.
Wright, J. C. (1959). Religion, sociability, and personal relations. Journal of Religious Education, 54, 521–523.
Wulf, J., Prentice, D., Hansum, D., Ferrar, A., & Spilka, B. (1984). Religiosity and sexual attitudes and behavior among evangelical Christian singles. Review of Religious Research, 26 (2), 118–131.
Young, R. K., Clore, G, & Holtzman, W. H. (1968). Further change in attitude toward the negro in a southern university. In D. Byrne & M. Hamilton (Eds.), Personality research: A book of readings. New York: Wiley.
