Health Practices and Cancer Mortality among Active California Mormons
James E. Enstrom
James E. Enstrom, “Health Practices and Cancer Mortality among Active California Mormons,” in Latter-day Saint Social Life: Social Research on the LDS Church and its Members(Provo, UT: Religious Studies Center, Brigham Young University, 1998), 441–460.
James E. Enstrom is research professor in the school of public health at the University of California at Los Angeles. This article was originally published in Journal of the National Cancer Institute 23:1807–14; reprinted with permission.
Abstract
Religiously active Mormons in California are a nonsmoking population with unusually low risk for cancer. This finding is based on the results of our 1979 questionnaire survey of life-style and the eight-year (1980–87) follow-up of mortality among 5,231 Mormon high priests and 4,613 wives 25–99 years of age. Our study, which is the first prospective cohort study of Mormons, shows low standardized mortality ratios (SMRs) for this population, relative to those for whites in the general population in the United States, which are defined as 100. The SMRs for males are 47 for all cancers, 52 for cardiovascular diseases, and 47 for all causes; the SMRs for females are 72 for all cancers, 64 for cardiovascular diseases, and 66 for all causes. For middle-aged high priests adhering to three health practices (never smoking cigarettes, engaging in regular physical activity, and getting proper sleep), the SMRs are 34 for all cancers, 14 for cardiovascular diseases, and 22 for all causes. These results have been largely replicated in an active Mormon-like subgroup (white nonsmokers attending church weekly) from a representative sample of residents of Alameda County, California. Our findings confirm and expand on previous descriptive studies of Mormons and demonstrate how these results can be generalized.
One means of gaining new insights into cancer etiology and prevention is to examine a well-defined low-risk population within the United States. It has been conclusively demonstrated (Enstrom 1975, 1978, 1980a, 1980b, 1983; Lyon, Klauber, Gardner, et al. 1976; Lyon, Gardner, and West 1980; Gardner and Lyon 1982) that members of The Church of Jesus Christ of Latter-day Saints, more popularly known as Mormons, constitute one such low-risk group. The Mormon church has about 4 million members in the United States and 6.5 million members worldwide, including about 500,000 in California and 1.2 million in Utah (The Church of Jesus Christ of Latter-day Saints 1989).
This population is interesting from an epidemiologic standpoint because its “Word of Wisdom” advises against the use of tobacco, alcohol, coffee, tea, and drugs (Enstrom 1975). Also, the religion emphasizes a strong family life and education, advocates good health practices in general, and recommends a well-balanced diet (Enstrom 1975).
Religiously active Mormons, specifically high priests, essentially abstain from tobacco, alcohol, and caffeine. We have studied this group because their cancer mortality rates are substantially lower than those of the general population and those of Mormons as a whole—a finding demonstrated in our previous studies (Enstrom 1978, 1980a, 1980b) and confirmed by other investigators (Gardner and Lyon 1982). High priests are long-term devout Mormons who have risen to the highest rank of the church’s lay priesthood, a rank they retain for the rest of their lives. Many of them currently serve on a voluntary basis as local church leaders. Their wives hold no priesthood level, but most are active Mormons as well. The number of high priests in California was about 16,000 as of 1 January 1980, and 25,000 as of 1 January 1988.
Previous research on cancer in Mormons has dealt with mortality in California and Utah (Enstrom 1975, 1978, 1980a, 1980b) and incidence in Utah (Lyon, Klauber, Gardner, et al. 1976; Lyon, Gardner, and West 1980; Gardner and Lyon 1982). These descriptive results have been based on church membership statistics, church death records, and records of newly diagnosed cases of cancer identified by religious affiliation. Life-style data on small samples of Mormons have confirmed that active Mormons do not smoke. However, abstention from smoking does not fully explain the descriptive cancer mortality patterns observed (Enstrom 1978). Consequently, we undertook a prospective epidemiologic study of a well-defined cohort of active Mormons.
This study provides the first detailed examination and explanation of the life-style characteristics of Mormons in relation to subsequent mortality rates. This detailed long-term assessment of the life-style of active Mormons as it relates to cancer mortality and minimum cancer risk provides new information regarding the actual prevention of cancer in a population in the United States.
Methods
Questionnaire
A four-page questionnaire to measure the life-style characteristics of active Mormons was prepared at the University of California, Los Angeles (UCLA). This questionnaire was sent around 1 December 1979, by Mormon church personnel, to high priests and their wives in California. To maintain the confidentiality of the members unwilling to participate, our questionnaires were mailed from the church headquarters in Salt Lake City, Utah, and willing respondents replied directly to UCLA. A letter accompanying the questionnaire made clear that the study was being done independently of the church.
A one-time mailing of two questionnaires (one for husband and one for wife) was made to about 12,000 California households of high priests with valid addresses on the church’s computerized membership file as of about 1 December 1979. Responses from 9,844 persons 25–99 years of age (5,231 high priests and 4,613 wives) were received at UCLA. The church did not permit additional mailings to nonrespondents.
The completed questionnaires provided data on basic demographic characteristics; major components of life-style, diet, and medical history; and other health-related characteristics. It incorporated parts of a 1974 Health and Ways of Living questionnaire used in Alameda County by the Human Population Laboratory of the California State Department of Health Services (Enstrom, Kanim, and Breslow 1986).
Mortality Follow-up
For all California high priests, including those in our cohort, complete and accurate mortality data have been obtained for eight years, from 1 January 1980 through 31 December 1987. We have obtained 1980–87 mortality data on all high priests in California from the Mormon church computerized membership file in Salt Lake City. To verify deaths and determine the underlying cause of death, we computer matched the church data on the deceased high priests with the data on all California deaths, matching on the full name, date and place of birth, and date and place of death of the deceased person. The underlying cause for each California death has been assigned by the state nosologist, following the rules of the ninth revision of the International Classification of Diseases (ICD9). The mortality data and the age-specific membership statistics obtained from the Mormon church have been used to calculate mortality rates for all Mormon high priests in California during 1980–87. These mortality rates update previously published rates for 1968–75 (Enstrom 1980a). Similarly, the data from the high priest cohort have been computer matched with the 1980–87 mortality data obtained from the files of the Mormon church and the state of California to identify all cohort deaths. We estimate that no more than 2 percent of all deaths in cohort members in California have been missed by matching with these two sources. We have identified 612 deaths of cohort members in California, but deaths of members who left the state have not been included.
We have used the California Department of Motor Vehicles (DMV) files to verify the vital status and current addresses of the high priests and to estimate their movement out of California. In 1980, 98 percent of cohort members and 99 percent of households were linked with the DMV driver’s license file. This file has been updated twice a year with notation made when individuals left California for another state or died. As of 1 January 1988, approximately 11 percent of the cohort members had left California, according to the DMV.
Comparison Group
To compare the high priest cohort with the general population, we made use of data on the 1974 representative sample of 3,119 noninstitutionalized adults in Alameda County, which has been used previously to study the relationship between health practices and mortality (Enstrom, Kanim, and Breslow 1986) and to make comparisons with Mormons (Enstrom 1980b). Alameda County is similar to the state of California and the United States as a whole in terms of population demographics and mortality rates.
Analysis
Our analysis of life-style is based on three general health practices:
(1) never smoked cigarettes;
(2) engage in regular physical activity (often or sometimes engage in active sports, swim, or take long walks or often garden or do physical exercises); and
(3) get proper sleep (usually 7–8 hr/
Standardized mortality ratios (SMRs) for major cancer sites, all cancers (ICD9 140–208), all cardiovascular diseases (ICD9 390–459), and all causes are calculated for the total cohort as well as for the health practice subgroups. SMRs are presented for persons in the 25–99-year age group during the study period and for persons in the 24–64-year age group at entry in the study.
The SMR for each subgroup is the number of observed deaths divided by the number of expected deaths, expressed as a percentage. The total number of expected deaths is the sum of the expected deaths for each five-year age group. The number of expected deaths for one five-year age group is the number of person-years of risk multiplied by the age-specific mortality rate for that age group of whites in the United States. The total person-years at risk are based on the person-years at risk among California residents. For each person, the period of risk began 1 January 1980 and ended on the date of death; date of leaving California according to the DMV; or 31 December 1987, whichever came first.
We calculated each SMR and its 95 percent confidence interval using a survival program developed by Monson (1974), with expected deaths based on concurrent death rates among whites in the United States. By this definition, the SMRs for whites in the general population in the United States are 100. We chose this population as the standard for comparison of mortality because detailed data are widely available and the mortality rates are similar to those for comparable groups, such as California whites or Alameda County whites. Because of the small number of deaths in some subgroups, SMRs, which are based on indirect age standardization, have been used instead of age-adjusted death rates, which are based on direct age standardization. However, the results by both methods are consistent. The age distribution in the high priest cohort at the time of enrollment was as follows: 7 percent for ages 25–34 years, 21 percent for ages 35–44, 28 percent for ages 45–54, 23 percent for ages 55–64, 14 percent for ages 65–74, 6 percent for ages 75–84, and 1 percent for ages 85–99.
Results
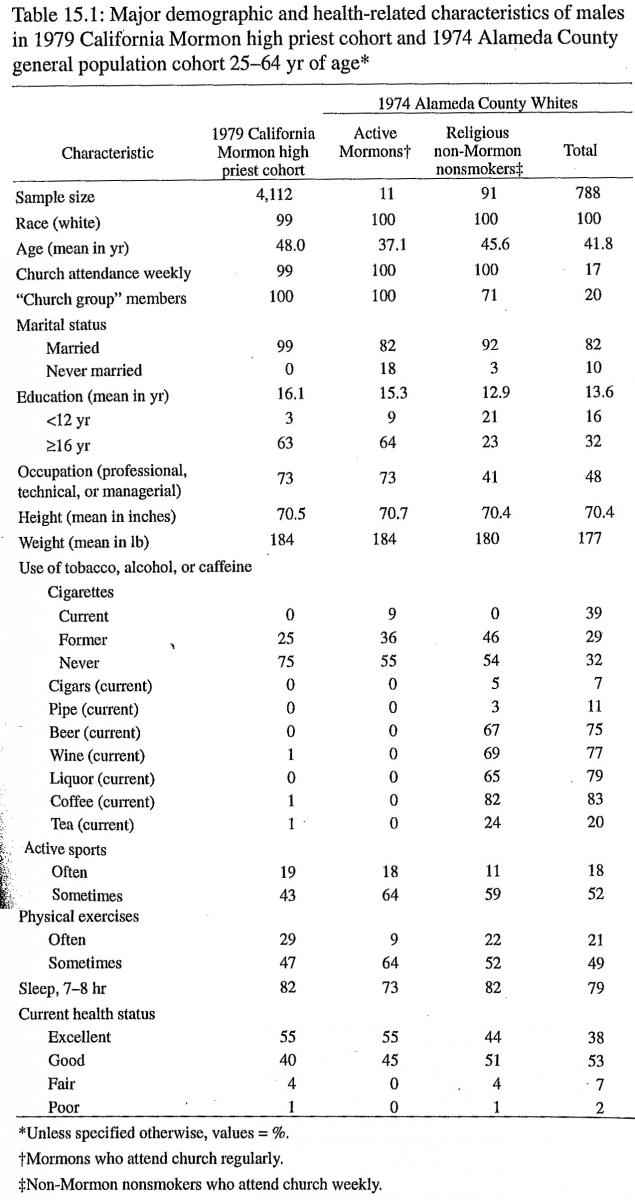
Several basic demographic and health-related characteristics of the 1979 California high priest cohort and the 1974 Alameda County representative cohort are shown in table 15.1 for males and in table 15.2 for females. These persons were 25–64 years of age at the time of entry. Data are presented for all whites in the Alameda County cohort and for two white subgroups: Mormons who attend church weekly and non-Mormon nonsmokers (former smokers and those who never smoked) who attend church weekly. The Alameda County Mormons were identified on the basis of their answers to the questions on religion and church attendance. There are only 27 of them, but within statistical fluctuation, their characteristics are similar to those of the high priest cohort. The high priests are white, married, and well educated; attend church weekly; and use essentially no tobacco, alcohol, or caffeine.
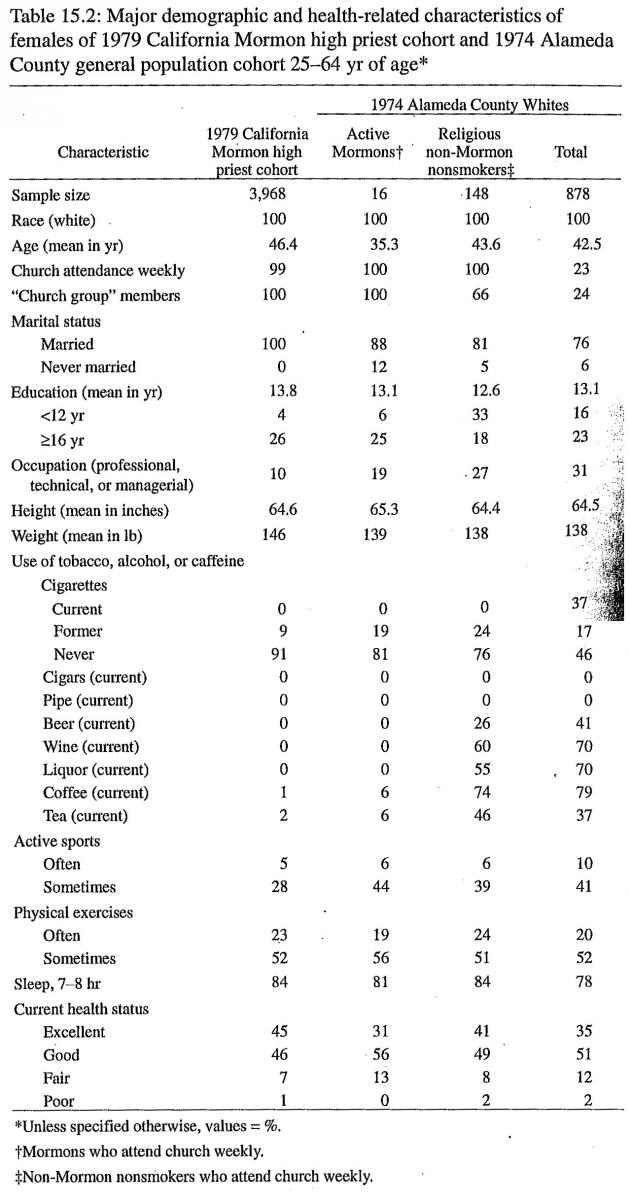
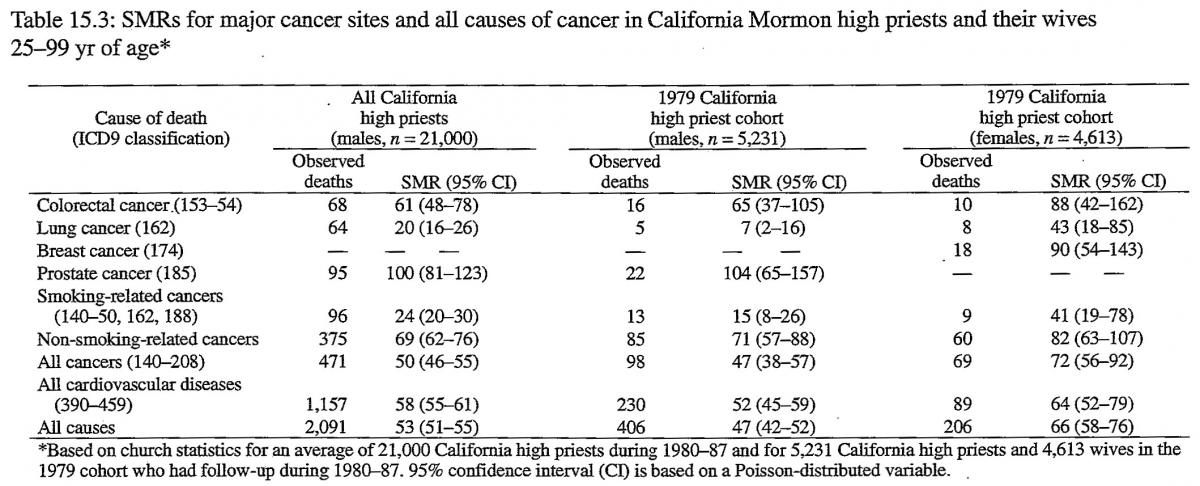
Table 15.3 shows that the SMRs during 1980–87 for an average of 21,000 California high priests are 50 for all cancers, 24 for smoking-related cancers, 69 for non-smoking-related cancers, and 53 for all causes. The SMRs during 1980–87 for 5,231 high priests from the 1979 cohort are 47 for all cancers, 15 for smoking-related cancers, 71 for non-smoking-related cancers, and 47 for all causes. The results for the high priest cohort are similar to those for all California high priests. The difference for lung cancer (7 vs. 20) may be due to the fact that there is a somewhat larger proportion of persons who never smoked in the cohort than among all California high priests. The small difference for all causes (47 vs. 53) may be due to a small questionnaire-respondent bias (see Discussion section).
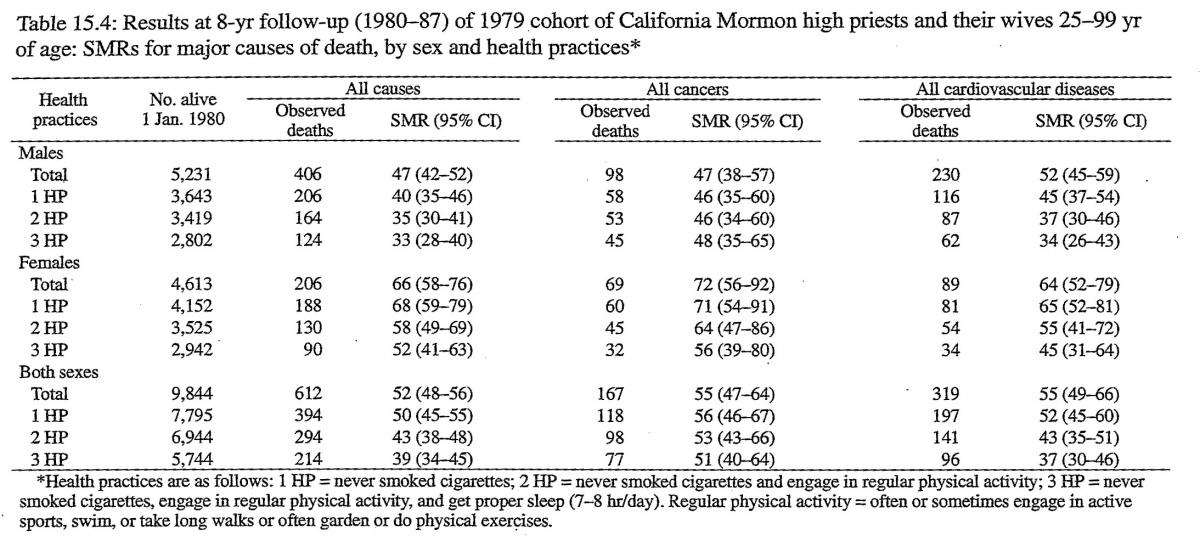
Table 15.4 shows the SMRs for all causes, all cancers, and all cardiovascular diseases for persons 25–99 years of age in the high priest cohort, by sex and the three health practices. The SMRs generally declined with adherence to more of these practices. The SMRs for all causes declined from 47 to 33 for males and from 66 to 52 for females. The SMRs for all cancers changed from 47 to 48 for males and from 72 to 56 for females. The SMRs for all cardiovascular diseases declined from 52 to 34 for males and from 64 to 45 for females. Several health practices other than the three we considered in our analyses were related to mortality in the Alameda County study (Enstrom, Kanim, and Breslow 1986; Kaplan, Seeman, Cohen, et al. 1987), but they had no additional impact on the SMRs for the high priest cohort. These additional practices were maintenance of proper weight for height, moderate alcohol consumption, eating breakfast, and not eating between meals. We have not yet explored all possible health and dietary practices in relationship to mortality, so it is possible that other combinations could have an impact on the SMRs.
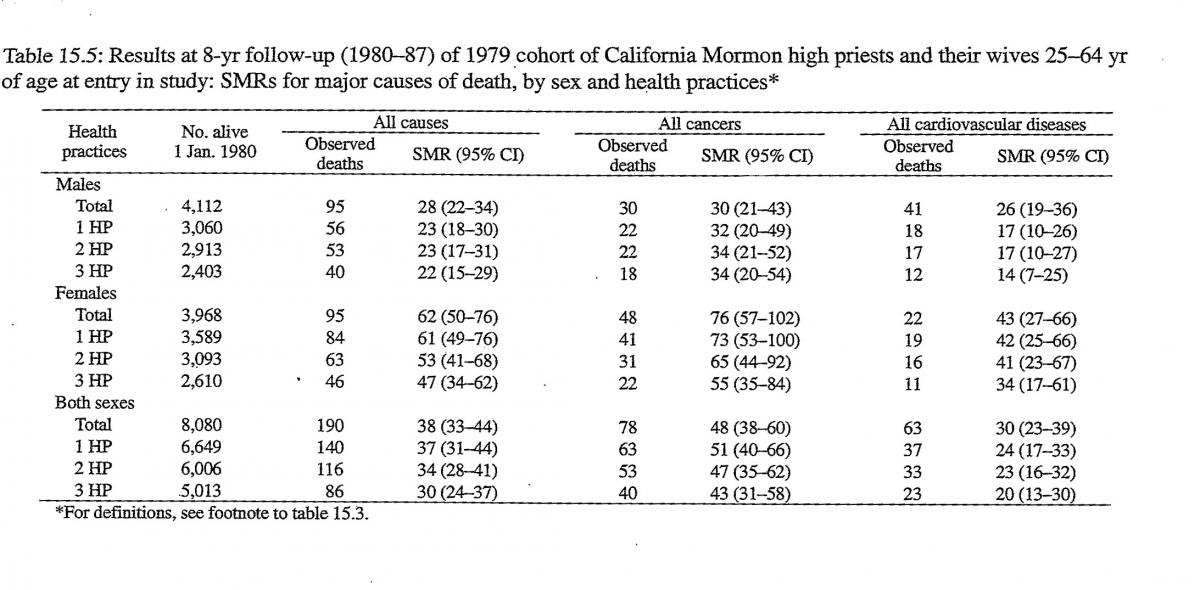
Table 15.5 shows the SMRs for persons in the high priest cohort who were 25–64 years of age at entry in the study. These SMRs are lower than those shown in table 15.4 for persons in the 25–99-year age group. The differences are large for males and small for females. For ages 25–64 years, the SMRs for males are 30 for all cancers and 28 for all causes, and the SMRs for females are 76 for all cancers and 62 for all causes. For persons adhering to the three health practices, the SMRs for all causes declined even further: from 28 to 22 for males and from 62 to 47 for females. The SMRs for all cancers did not vary significantly with the number of health practices, but the SMRs for all cardiovascular diseases declined substantially: from 26 to 14 for males and from 43 to 34 for females.
To see the extent to which these results can be reproduced in the general population, we analyzed the 1974 representative sample of noninstitutionalized Alameda County residents (Enstrom, Kanim, and Breslow 1986) for residents with characteristics similar to those of active Mormons. We defined “active Mormon-like” persons as residents of all religions who are white, do not smoke cigarettes (former smokers and those who never smoked), and attend church weekly. Their SMRs for all causes were 42 for males and 61 for females, as shown in table 15.6. The SMRs for all whites, whites who never smoked cigarettes, active Mormon-like persons, and active Mormon-like persons with the three health practices are presented in table 15.6 for all causes, all cancers, and all cardiovascular diseases. The SMRs for active Mormon-like persons in the Alameda County cohort are the same as the corresponding SMRs for the high priest cohort (table 15.4), within statistical fluctuation. Although the data are not shown in table 15.6, the SMRs for all Alameda County whites were substantially less than 100 during the first five years of follow-up, but thereafter, the values were about 100, as the effect of initially including only noninstitutionalized persons diminished.
Logistic regression analyses of data from the Alameda County cohort show that the associations of mortality with age, sex, initial health status, cigarette smoking status, and frequency of church attendance are statistically significant (P<.05). Several additional variables, such as race, marital status, education level, and other health practices were not significant in the regression analyses after the first five variables were accounted for. Thus, the overall SMRs for the high priest cohort appear to be reasonably well explained by the fact that the cohort consists of white nonsmokers who attend church weekly. The analyses are not exhaustive, however, and other variables may be significant. For instance, weekly church attendance may be related to other variables yet to be determined.
Discussion
These findings indicate that active Mormons (high priests and their wives) have very low rates of mortality from all cancers and all causes. The plausibility of these findings is supported by related research.
Church attendance has previously been associated with reduced mortality in a sample of the general population in Maryland (Comstock and Partridge 1972; Comstock and Tonascia 1977) and in a few other populations (Levin and Vanderpool 1987). For many decades, reduced mortality rates have been reported among clergy (King and Locke 1980; King and Bailar 1969) and among health-conscious religious groups, such as Seventh-Day Adventists (Phillips 1975) and Mormons (Enstrom 1975). Although high priests are lay clergymen, they may be similar in many ways to formal clergymen. Also, these results may be partially influenced by the strong social network ties among high priests, who are all married and belong to a church group. Social networks have previously been related to total mortality, independently of other health practices (Seeman, Kaplan, Knudsen et al. 1987; House, Landis, and Umberson 1988).
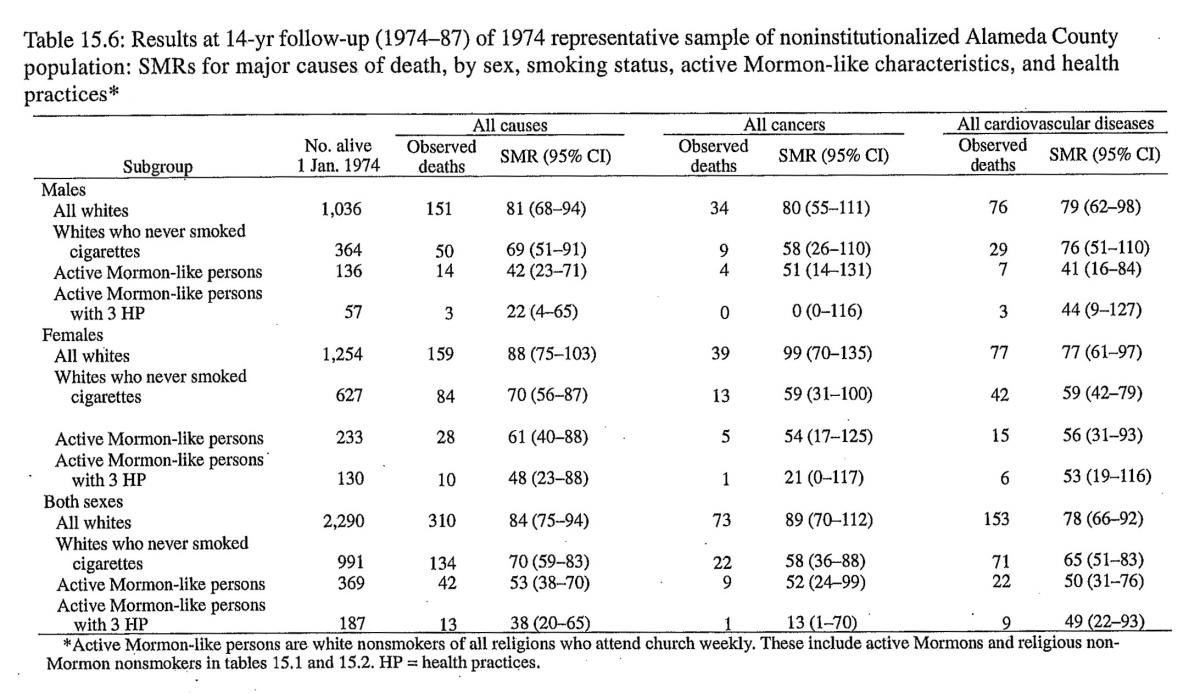
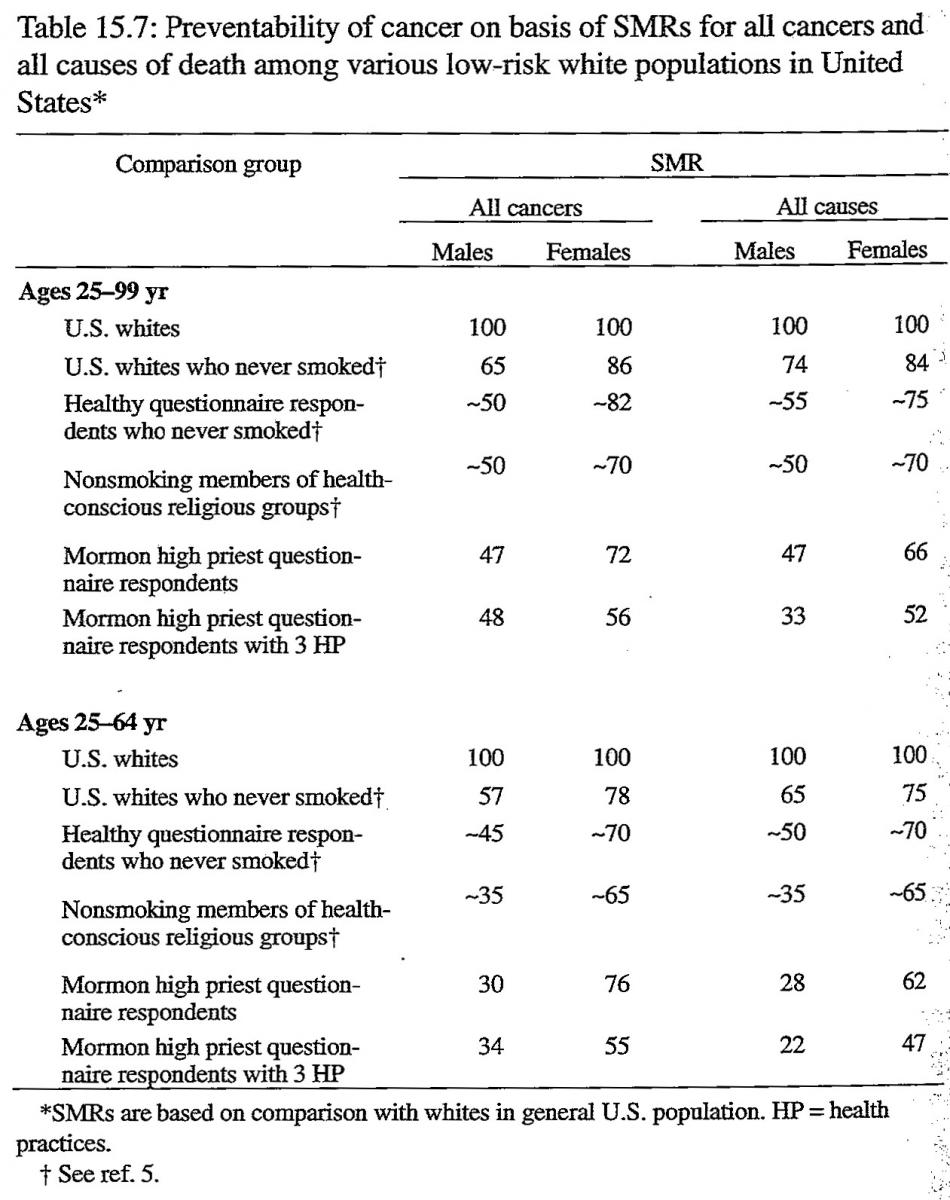
Table 15.7 shows a comparison of SMRs for all cancers and all causes in major low-risk populations in the United States. These populations are whites who never smoked, healthy questionnaire respondents who never smoked, nonsmoking members of health-conscious religious groups, Mormon high priest questionnaire respondents, and a subgroup of these high priests with the three health practices. Except for our data for high priests from this study, the data on these low-risk populations are derived from other major epidemiologic studies during the past 35 years (Enstrom and Kanim 1983). The SMRs are based on comparison of each low-risk population with whites in the United States. The SMRs for all high priests are in agreement with those for nonsmoking members of health-conscious religious groups. However, for high priests with the three health practices, the SMRs for cardiovascular diseases and all causes are among the lowest ever reported.
To strengthen the validity of our findings, we have carefully examined three factors that could cause spurious results: underascertainment of deaths, selection bias due to the number of healthy questionnaire respondents, and unique results applicable only to the cohort. First, there is virtually complete ascertainment of our data on California deaths, because we have obtained consistent and overlapping reporting of deaths from three independent sources: California death files, Mormon church death files, and California DMV death records. In addition, dates of birth given on the questionnaires are in agreement with those on the DMV records, indicating that the age distribution is correct. Also, movement of cohort members from California has been accounted for by careful monitoring of driver’s license records.
Second, there is little evidence that the SMRs were unusually low because of bias due to the number of healthy questionnaire respondents. This selection bias occurs when only the healthiest persons respond to a questionnaire mailed to a target population. The result is extremely low SMRs in the first few years of follow-up, followed by SMRs that steadily increase until the bias is no longer significant. But for our cohort, the SMRs have remained fairly constant in years one to eight of follow-up. The SMRs for all causes, by year, are 44, 48, 40, 42, 48, 49, 47, and 56 for males and 78, 63, 57, 42,68,61,74, and 90 for females. In addition, the SMRs for all causes are stable over the eight-year follow-up period when analyzed by the three health practices and by age at entry in the study. Also, the SMRs for the prospectively followed high priest cohort are in good agreement with concurrent SMRs calculated independently from Mormon church death records and membership statistics for all high priests. In addition, the SMRs agree with previously published descriptive mortality data on high priests (Enstrom 1978, 1980a, 1980b; Garder and Lyon 1982). We believe the respondent bias is small, because high priests as a whole are such a healthy group and because our cohort includes a representative sample of them, even though the response rate to the one questionnaire mailing was not particularly high.
Third, the findings in our high priest cohort have been replicated to a large extent in a representative sample of the general population. Thus, these findings are not unique to our cohort; they are generalizable.
Conclusions
For high priests, especially those who are middle-aged, the SMRs for all cancers, for cardiovascular diseases, and for all causes are substantially below those for typical nonsmokers. Indeed, this population is currently achieving the 50 percent reduction in cancer mortality that the National Cancer Institute has set as a goal for the year 2000 (Breslow and Cumberland 1988). These results demonstrate substantial progress in prevention of cancer and other diseases in one well-defined population, and they suggest a life-style that could result in a major reduction in cancer mortality, as well as mortality in general. Further research might reveal that additional health practices result in an even greater reduction in mortality.
References
Breslow, L. and W. G. Cumberland. 1988. “Progress and Objectives in Cancer Control.” Journal of the American Medical Association 259:1690–94.
Church of Jesus Christ of Latter-day Saints. 1989. 1989 Church Almanac. Salt Lake City: Deseret News.
Comstock, G. W. and K. B. Partridge. 1972. “Church Attendance and Mortality.” Journal of Chronic Diseases 25:665–72.
Comstock, G. W. and J. A. Tonascia. 1977. “Education and Mortality in Washington County, Maryland.” Journal of Health and Social Behavior 18:54–61.
Enstrom, James E. 1975. “Cancer Mortality among Mormons.” Cancer 36:825–41.
———. 1978. “Cancer and Total Mortality among Active Mormons.” Cancer 42:1943–51.
———. 1980a. “Cancer Mortality among Mormons in California during 1968–75.” Journal of the National Cancer Institute. 65:1073–82.
1980b. “Health and Dietary Practices and Cancer Mortality among California Mormons.” Pp. 69–92 in Banbury Report 4: Cancer Incidence in Defined Populations, edited by John Cairns, Joseph L. Lyon, and Mark Skolnick. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory.
Enstrom, James E. and Linda E. Kanim. 1983. “Populations at Low Risk.” Pp. 49–78 in Cancer Prevention in Clinical Medicine, edited by G. R. Newett. New York: Raven.
Enstrom, James E., Linda E. Kanim, and Lester Breslow. 1986. “The Relationship between Vitamin C Intake, General Health Practices, and Mortality in Alameda County, California.” American Journal of Public Health 76:1124–30.
Gardner, John W. and Joseph L. Lyon. 1982. “Cancer in Utah Mormon Men by Lay Priesthood Level.” American Journal of Epidemiology 116:243–57.
Hammond, E. C. 1964. “Smoking in Relation to Mortality and Morbidity. Findings in First Thirty-four Months of Follow-up in a Prospective Study Started in 1959.” Journal of the National Cancer Institute 32:1161–88.
House, J. S., K. R. Landis, and D. Umberson. 1988. “Social Relationships and Health.” Science 241:540–45.
Kaplan, G. A., T. E. Seeman, R. D. Cohen, et al. 1987. “Mortality among the Elderly in the Alameda County Study: Behavioral and Demographic Risk Factors.” American Journal of Public Health 77:307–12.
King, H. and F. B. Locke. 1980. “American White Protestant Clergy as a Low-Risk Population for Mortality Research.” Journal of the National Cancer Institute 65:1115–24.
King, H. and J. C. Bailar III. 1969. “The Health of the Clergy: A Review of Demographic Literature.” Demography 6:27–43.
Kripke, D. F, R. N. Simons, L. Garfinkel, et al. 1979. “Short and Long Sleep and Sleeping Pills: Is Increased Mortality Associated?” Archives of General Psychiatry 36:103–16.
Levin, Jeffrey S. and H. Y. Vanderpool. 1987. “Is Frequent Religious Attendance Really Conducive to Better Health?: Toward an Epidemiology of Religion.” Social Science and Medicine 24:589–600.
Lyon, Joseph L., M. R. Klauber, John W. Gardner, et al. 1976. “Cancer Incidence in Mormons and Non-Mormons in Utah, 1966–1970.” New England Journal of Medicine 294:129–33.
Lyon, Joseph L., John W. Gardner, and Dee W. West. 1980. “Cancer Incidence in Mormons and Non-Mormons in Utah during 1967–75.” Journal of the National Cancer Institute 65:1055–61.
Monson, R. R. 1974. “Analysis of Relative Survival and Proportional Mortality.” Comparative Biomedical Research 7:325–32.
Paffenbarger, R. S. Jr., R. T. Hyde, A. L. Wing, et al. 1986. “Physical Activity, All-Cause Mortality, and Longevity of College Alumni.” New England Journal of Medicine 314:605–13.
Phillips, R. L. 1975. “Role of Lifestyle and Dietary Habits in Risk of Cancer among Seventh-Day Adventists.” Cancer Research 35:3513–22.
Seeman, T. E., G. A. Kaplan, L. Knudsen, et al. 1987. “Social Network Ties and Mortality among the Elderly in the Alameda County Study.” American Journal of Epidemiology 126:714–23.
