Treatment Outcome
Debra Theobald McClendon, "Treatment Outcome," in Freedom From Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Provo, UT: Religious Studies Center, Brigham Young University; Salt Lake City: Deseret Book), 283–320.
Is Psychotherapy Effective for Treating OCD?
Before the 1960s, OCD was considered unresponsive to treatment. At that time OCD treatment mainly utilized psychoanalytic and supportive approaches. However, with the introduction of exposure and response prevention (ERP) in the 1960s, outcomes began to improve. Since then, many research studies, both controlled and uncontrolled, have established ERP, and cognitive behavioral therapy (CBT) more broadly, as a highly effective treatment for OCD.[1]
There have been many research studies examining the effectiveness of psychotherapy treatments for OCD. As such, researchers have sought to summarize results from multiple similar studies using meta-analyses. Meta-analyses report findings relative to effect size. “Effect size is a quantitative measure of the magnitude of the experimental effect. The larger the effect size the stronger the relationship between two variables.”[2] The following are findings from several meta-analytic studies,[3] presented in chronological order with the oldest study first:
- In a meta-analysis of treatment outcome studies, researchers found ERP to be highly effective in reducing OCD symptoms. Cognitive approaches were also found to be as effective as ERP.[4]
- One study found that effect sizes for ERP were significantly greater than medication (serotonin reuptake inhibitors) for the treatment of OCD.[5]
- Researchers later compared the effect sizes for cognitive therapy, ERP, and their combination (CBT) for the treatment of OCD. Similar effect sizes were found in these treatment conditions, although they were slightly stronger for the ERP and CBT conditions. Across all treatment conditions, about two-thirds of those who completed treatment improved.[6]
- Another meta-analysis also found that cognitive therapy, ERP, and their combination (CBT) were very effective in reducing OCD symptoms. The three conditions showed similar effectiveness.[7]
- A study with sixteen randomized controlled studies found that CBT outperformed control measures such as relaxation, anxiety management training, and pill placebo in reduction of OCD symptoms at the end of treatment and at follow-up, yielding a large mean effect size of 0.92.[8] That means CBT groups had a meaningful practical advantage over control groups.
Is CBT Treatment a Cure for OCD?
I am passionate about psychotherapy treatment for those suffering with scrupulosity. I have seen people reclaim their lives from OCD! Yet I recognize that CBT is not a cure for OCD. Despite the effectiveness of CBT, and significant improvement in the quality of clients’ lives, not all clients experience a full recovery or cure from OCD symptoms.
A meta-analytic review of sixteen controlled studies of ERP for adults with OCD indicated that the average symptom reduction across studies was 48 percent.[9] Other researchers have estimated that as many as 25 to 50 percent of clients discontinue treatment prematurely or experience relapse.[10] In a review of controlled and open trials of CBT for children with OCD, researchers noted that despite clinically significant reductions in OCD symptoms following treatment, between 50 to 75 percent of clients remained symptomatic following a full treatment course.[11] Clients may make significant, life changing, and even miraculous improvements with CBT, but they may continue to have some lingering issues. In these cases the OCD becomes much easier to manage overall, with the person enjoying more emotional freedom to engage more abundantly in daily life, but the OCD may still create some “background noise.” One client illustrated this dynamic while exploring her recovery process:
It is hard to describe how much control of my life I have gained back. Since I have been in therapy, I’ve grown a lot and gained my happiness back. I’m beyond grateful for the quality of life that I am able to live. That being said, scrupulosity OCD has a way of finding the cracks and capitalizing on them. I find myself having repetitive thoughts about things a friend, professor, or family member said. I worry about minuscule things that my scrupulosity latches on to. I obsess about doing the “right” thing and when I’ve done the “wrong thing.” I cycle through scrupulous topics that I’ve already beaten to the ground. Thankfully these experiences no longer control my life, and they have taken a back seat. Finding joy and peace is possible. Keep pushing.
Do Outcomes Vary for Different OCD Forms?
A study using an inpatient population (meaning the baseline symptom presentation for the clients was more severe and complex than usual) examined the effectiveness of psychotherapy treatment for various OCD subtypes. Researchers found that ERP was effective for all obsessive-compulsive symptom dimensions, yet those inpatients with hoarding symptoms responded most poorly to CBT treatment.[12] They also found that those with sexual and religious obsessions responded to treatment less frequently than other subtypes, although this was not a statistically significant finding (P = 0.07).
A later study reviewing multiple treatment studies found that scrupulosity (specified as sexual and religious obsessions) tended to be more difficult to treat, with studies producing mixed results.[13] If desired, you may want to review chapter 8’s discussion about treatment difficulties in scrupulosity for some of the clinical issues that may contribute to this finding.
Do Demographics Influence Treatment Outcome?
Demographic characteristics do not appear to impact treatment outcome for those with OCD. Age of onset is not a consistent predictor of treatment outcome. Most OCD treatment studies examining how current age affected treatment for adults found that age was not predictive of treatment response,[14] although one study found that a younger age was predictive of better outcome at posttreatment and follow-up. In a pediatric study, age was also not predictive of treatment response.[15] Gender also does not seem to consistently affect treatment response. Although some studies have found minor gender differences, the majority of studies have failed to find support for those differences.[16]
Co-occurring Mental Illnesses
Some research has found that those suffering with OCD who also struggle with severe depression tended to have poorer treatment outcomes. Researchers suggested that the depression was predictive rather than just associative—the depressive symptoms (e.g., anhedonia, feelings of hopelessness) interfere with the person’s ability to work a therapy program effectively. In those cases, researchers have suggested that targeting the depression specifically in psychotherapy may improve treatment response.[17]
A more recent meta-analysis combining sixteen randomized controlled trials (RCTs) showed that depression symptom severity was not significantly associated with a decrease in CBT effect size. However, this should be interpreted with caution because “the samples used in RCT research may not always be representative of the OCD population at large. This may be especially relevant for examining the extent to which depression predicts outcome. Indeed, RCTs often exclude very depressed patients (in order to maximize internal validity), which restricts the range of depression severity in these studies, potentially obscuring relationships with outcome.”[18]
Number of Sessions Needed to Effectively Treat Scrupulosity
Psychotherapy is an effective process generally. For people without OCD, those attending general psychotherapy or counseling may often be effectively treated for their difficulties within eight to fourteen sessions.[19] It is a more protracted process for severe difficulties or those with co-occurring disorders. Therefore, OCD treatment length may be longer, taking about twelve to twenty sessions (again, making allowance for more complex cases needing a longer treatment process).
With the many treatment complexities involved in treating scrupulosity, one should expect a longer treatment process than it would take to treat other forms of OCD (except perhaps hoarding). Violating expectations related to the uncertainty in scrupulous fears is a process that “may simply proceed more gradually than violating threat overestimations related to more immediate, tangible outcomes.”[20]
For example, in my outpatient private practice, mild cases of scrupulosity are effectively treated within five to twelve sessions, with an average of nine sessions. Those suffering with a moderate level of scrupulosity (and did not prematurely end their therapy) have been effectively treated in about thirty to forty sessions. Few clients with a severe level of scrupulosity have completed therapy at my practice since it operates on an outpatient basis (typically seeing people once per week). For them, most either ended therapy prematurely or were escalated to a higher level of treatment for more intensive care (i.e., they were referred to an intensive outpatient program). For those with severe scrupulosity who do complete therapy in my outpatient private practice, it generally takes more than sixty-six sessions.
Spacing of Therapy Sessions
Therapy sessions are typically arranged to be more frequent at the beginning of treatment, and then spaced further apart near the end of treatment, to promote self-reliance and consolidation of gains. You may generally plan to meet with a mental health professional on a weekly basis for three to six months, then every other week for another few months, and then meet only monthly. A couple months later you may opt for a booster or check-in session. I often suggest that clients think about maintaining on ongoing therapeutic relationship with their therapist that is similar to what is seen in dentistry—once you conclude your more regularly scheduled therapy appointments, consider checking in with your therapist every six months or so. I find that the clients who make this a priority maintain their therapeutic gains and are more resistant to relapse.
Self-Reported Lifestyle Benefits of Psychotherapy
What types of benefits might you receive from engaging in scrupulosity treatment? In addition to a reduction of distress and diminished fear to anxiety triggers, there are many other lifestyle improvements you might enjoy. One client who had been in treatment for some time and had made significant progress needed to rebuild his motivation and commitment to therapy when his life got particularly stressful and busy. He outlined benefits he had already seen from working diligently at his therapy. He was surprised to see the benefits extend far beyond just his original treatment goals. See what he produced in figure 14.1.
Client Stories of Therapeutic Progress
Four Treatment Outcome Examples, with Data
Here I share with you four clients who tell their stories about their journey through scrupulosity treatment. This may give you an idea of what therapeutic progress may look like for different people. Keep in mind these are clients working through their scrupulosity treatment while also managing the rest of their activities; they are not inpatients or subjects in a controlled research study. For example, many of my clients are busy university students who may struggle to get enough therapy or exposure work done, especially during midterm and finals weeks. Considering these real-world circumstances, the improvements these clients experienced are impressive (and yet, not unusual).
Example 1. The first client example is a college-age male presenting to therapy for scrupulosity treatment. He had recently returned from serving as a missionary for The Church of Jesus Christ of Latter-day Saints. Here is his story:
My problems with scrupulosity developed when I was about seventeen years old. I had toclearthingsupsothatIcouldgetreadyformymissionandwasconfessingthingsthatIneededto.Iwouldgointothebishop’sofficeandconfesssome times multiple times in a week, not all new sins, but a lot of describing the sins that I had made in more detail. I also saw accidents as some thing that I needed to confess. I then never got to the spot where I could consider myself clean or worthy.
The stuck point was that I would need to get to a bishop or stake president for approval, which was once a week on the mission [with my mission president]. I didn’t have certainty until they told me I was “ok.” I would email [my mission president] every week, and before I could even see my reply in the next week, I would have more things to confess. I always considered that I would be worthy once I got the next things cleared up. I was stuck with ideas that I may have done something really bad, even for a second, as in gay actions or with kids, that would not allow me to be worthy for years to come. I could not get full confirmation that I had not done these things, and I could not accept the uncertainty. I was also stuck with not being able to know if the bishop and stake president, or whoever I confessed to, had completely understood my confession. That is why I continued to describe my confessions to them. I would often “overconfess” just to make sure that I got everything off of my chest and that they understood the gravity of my wrong actions.
I felt like I was never going to get clean, that I had maybe done something for which I could never become clean and/
or married in the temple and have a future. I felt like I needed to go to heaven and deal with Heavenly Father and was terrified of being taken away from my loved ones at judgment day. I was very, very suicidal on the mission. I saw my life as a failure and that I would need to die because I could never accomplish the dreams I wanted to accomplish or live with the guilt I had. It was very hard to move forward.
His main anxiety triggers were issues around honesty and sexual purity and chastity. You can see how he completed his fear hierarchy in table 14.2. Every trigger provoked very high levels of anxiety, with nothing even listed on his hierarchy below a seven.
Table 14.2. Client example 1: Fear hierarchy
SUDs | Triggering Situation |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| 7 | • Honesty • Past sins • Exact obedience (tithing on investments) |
| 8 | • Sexual thoughts • Accidental contact with private body parts |
| 9 | • Honesty/ |
| 10 | • Perfect confession |
Figure 14.3 shows you his treatment outcome assessment data.
Figure 14.3. Client example 1: Outcome measures (OQ-45.2 and PIOS-R)
In this chart there are two outcome measures that assess the client’s treatment progress: the Outcome Questionnaire (OQ-45.2) and the Pennsylvania Inventory of Scrupulosity-Revised (PIOS-R). As you look at the x-axis of this chart, you will see dates that correspond to this client’s therapy sessions. We met weekly for the first six sessions, and then about every other week, and then had a month between the last two appointments. We had a total of twelve therapy sessions.
The first thing I want you to notice about this chart is the client’s OQ-45.2 score on the y-axis. The average score on the OQ-45.2 for a community sample (those that are not in therapy or needing clinical intervention) is 45. Since his initial OQ-45.2 score is 37, the client was already functioning in the average range when he began therapy. He was functioning pretty well in general except for his struggles with scrupulosity. It is not uncommon for someone struggling with an isolated therapeutic issue to present to therapy with an OQ-45.2 score in the average range since the questions highlight a broad range of issues. Second, take note on the y-axis that the clinical cutoff score for the PIOS-R is 24 (out of 60).[21] This means any score of 24 and above indicates that the person is struggling with high distress that creates significant interference from scrupulosity in his or her life. This level of distress warrants targeted treatment, while any score 23 and below is subclinical and would be considered in the normal or average range. This client’s initial score on the PIOS-R was 37. Although the PIOS-R does not have delineated severity categories, such as mild, moderate, or severe, based on my clinical experience I would consider this a moderately high level of scrupulosity. [22]
As you examine this chart, you can see with the OQ-45.2 that even though he started therapy in the average range, he still made therapeutic gains in his overall life functioning. The OQ-45.2 is a general distress measure, so you can see how his distress continued to go down throughout treatment. He ended therapy with an OQ-45.2 score of 21, which I would consider superior functioning. Focusing treatment on his scrupulosity, you can see by his PIOS-R scores that it took a few sessions to start to see progress (which is typical), and then you see his scores drop. He ended therapy with a PIOS-R score of 11, well within the subclinical or average range.
During our tenth session, he indicated that nothing was bothering him much at that point. So we adjusted his hierarchy of fears to reflect the shifts in his fear. You can see a dramatic drop on the hierarchy. Before therapy everything provoked anxiety at level 7 or higher. In this chart nothing is ranked higher than a 6. In addition, these triggers were happening very infrequently for him at that point. When something did come up, he had the skills to be able to work through it effectively.
Table 14.4. Client example 1: Client’s adjusted fear hierarchy
| SUDs | Triggering Situation |
| 1 | |
| 2 | • Accidental contact with private body parts |
| 3 | • Past sins |
| 4 | • Perfect confession • Honesty |
| 5 | • Exact obedience (tithing on investments) |
| 6 | • Sexual thoughts • Honesty/ |
| 7 | |
| 8 | |
| 9 | |
| 10 |
Some years after completing therapy, this client reflected:
The first part of starting on my road to recovery was identifying the issue. Once I learned that what I was feeling was not just the loss of the Spirit, but was actually a mental illness, that helped me a lot just through comfort. I was then able to identify what steps I could take using professional help. The professionals helped me even more to identify what I was going through, which then allowed me to work through them. I think the key to my continuing progression has been awareness. When I am able to identify my thinking patterns as scrupulosity, I can work toward moving forward.
The most important thing for my recovery was being able to identify what is and what is not scrupulosity, or more just accepting the uncertainty around that question. I often am now able to identify when my thoughts are impulsive, unreasonable, and sudden, which shows me that they are anxious thoughts. I learned in therapy that those are characteristics of anxiety, not the Spirit. Even when I think something is real, I am usually able to identify the impulsive feeling that comes with it. Sometimes I just have to accept the uncertainty that maybe the thought is real, and then move forward with it. This usually leads to it subsiding. (The characteristics of Anxiety vs. the Spirit chart I believe was what I found super helpful here.)
I have been recently married and have been able to learn what I want for my wife and future children. This has simply led to me trying to be my best self. Even though I still face negative OCD thoughts, I know that I always need to do my best to be my best for my family. This leads to me accepting uncertainty and moving forward, rather than dwelling on the past and lacking progression.
Dealing with scrupulosity is a journey. Although I don’t really believe that my thought patterns will change, I am learning how to better identify and deal with them. Scrupulosity is the hardest thing I have ever been through by far. It makes you feel that you are worthless with no escape, even in the eternities to come. Be patient with yourself and do everything you can to accept uncertainty. Lots of the time you will not want to accept that maybe something you believe is true is actually true, but that is the only way through it. The first times are the hardest. Also, the Atonement of Jesus Christ is amazing. Even though you may have talked yourself (like I have) to a place that leads you to believe that you have maneuvered around the saving power of the Atonement, it is infinite. It was designed to heal everyone, even those who truly believe that they are far from its saving powers. Scrupulosity is a war, but as you learn more and more about it and how it really is OCD, it is incredibly healing and will allow you to live your life again!
Example 2. The second client example is also a college-age male, presenting to therapy for scrupulosity treatment. He had also recently returned from serving as a missionary for The Church of Jesus Christ of Latter-day Saints. His distress levels were quite a bit higher than in the previous example.
In hindsight, I now clearly recognize obsessive-compulsive tendencies in my childhood, but my formal problems with scrupulosity began on my mission for The Church of Jesus Christ of Latter-day Saints. I felt utterly unworthy to represent the Savior each and every day. I remember feeling as if the weight of damnation had rested upon my shoulders, and that I was barred from forgiveness from and connection with God. I began giving into scrupulous obsessions and compulsions. Every day was tainted with hours of ruminating thoughts fueling my anxiety concerning my worthiness and value before God. I set up multiple appointments with my mission president to confess every sin I could remember committing. Giving into these compulsions only made things worse. Scrupulosity hijacked my spiritual experience and mission.
During the peak of my experience with scrupulosity, I fell into the trap of erroneously thinking that spiritual actions could fix a psychological condition. Further, overcoming ruminating thinking was one of my greatest challenges with scrupulosity.
I felt hopeless, alone, abandoned, terrified, and damned. But worst of all, I felt that I deserved it. I felt that I was truly unworthy and undeserving of love from God and my loved ones.
When we met, this client’s main anxiety triggers centered on overthinking or ruminating on social situations, academic perfectionism, and church-related fears. You can see how he completed his fear hierarchy in table 14.5.
Table 14.5. Client example 2: Fear hierarchy
SUDs | Triggering Situation |
| 1 | • Reading scriptures (or something good that is getting touched by anxiety) |
| 2 | • Partaking of the sacrament |
| 3 | • Giving a priesthood blessing |
| 4 | • Platonic relationship situation of overthinking • Worry about being judgmental about someone else’s level of religious involvement |
| 5 | • Performing a live baptism • Lessons from church on repentance and law of chastity |
| 6 | • Anxiety of getting canceled • Romantic relationships/ • Reading patriarchal blessing—idea that I have disqualified myself for the blessings promised |
| 7 | • Remembering past transgressions • Going to the temple • Accidentally referencing the temple in casual conversation |
| 8–9 | • Romantic social situations overthinking romantic relationship: constant replay in mind • Academic perfectionism |
| 10 | • Anticipating getting sealed in the temple someday |
Figure 14.6 shows you his treatment outcome assessment data.
Figure 14.6. Client example 2: Outcome measures (OQ-45.2, PIOS-R, and Y-BOCS)
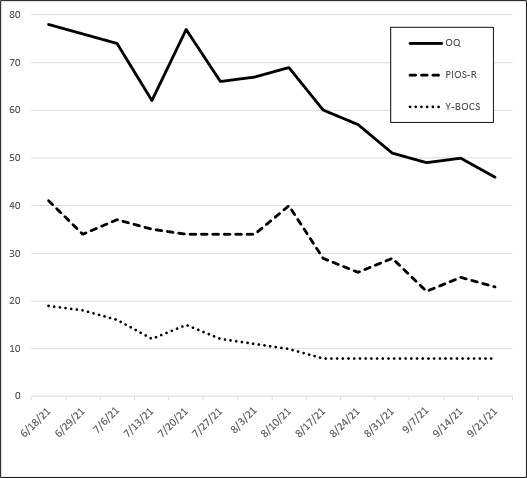
Three outcome measures track the client’s treatment progress: the OQ-45.2, the PIOS-R, and the Yale Brown Obsessive-Compulsive Scale (Y-BOCS). As you look at the x-axis on this chart you will observe dates that correspond to his therapy sessions. This chart represents the first fourteen sessions, meeting weekly. The first thing I want you to notice about this chart is the client’s highest score on the y-axis, the OQ-45.2 score. Remember, the average score on the OQ-45.2 for a community sample is 45. So the first thing you can notice here is that, with an initial OQ-45.2 score of 88, this client was struggling significantly. Indeed, this is the type of score that is typically seen when a person presents for outpatient psychotherapy treatment. Second, take note on the y-axis that the clinical cutoff score for the PIOS-R is 24 and this client’s initial score on the PIOS-R was 41. Based on my clinical experience, I would consider this a moderately high level of scrupulosity.[23] Third, the client also was administered the Y-BOCS, a general OCD severity measure. His initial Y-BOCS score for session one, seen along the y-axis, was 19. According to Y-BOCS researchers, 19 represents a moderate level of clinical OCD disturbance in someone’s life.[24]
As you examine this outcome-measure chart for this client, you can see that his scores shifted up and down a bit over the first seven sessions, and then all of the scores dropped significantly when he took the measures before the start of session eight. They all stayed low from that point on. With the OQ-45.2 he crossed the clinical threshold (clinical cutoff is a score of 63) briefly at session four and then popped back up. After his eighth therapy session, he then crossed again between the clinical and nonclinical range, never to experience increased distress at that level again. The OQ-45.2 is a general distress measure, so you can see here that his distress continued to go down throughout treatment. This chart ends with his OQ-45.2 score at 46, solidly within the average, nonclinical range. Examining his PIOS-R scores, you can see that after some ups and downs, his scores drop (also after that eighth session). This chart ends showing a PIOS-R score of 23, just under the clinical cutoff of 24. The Y-BOCS score also changes significantly. His Y-BOCS was 19 at session one; it also dropped significantly after session eight, holding strong at a score of 8. An 8 on the Y-BOCS is a mild score,[25] but it is only one point above the subclinical, or normal range, indicating that his OCD was not significantly interfering in his life at this point.
As we continued to meet, we kept refining our work through his areas of difficulty. His scores remained low. During our thirtieth session, we adjusted his hierarchy of fears to reflect the shifts in his fear. See table 14.7.
Table 14.7. Client example 2: Client’s adjusted fear hierarchy
| SUDs | Triggering Situation |
| 1 | • Reading scriptures (or something good that is getting touched by anxiety) |
| 2 | • Partaking of the sacrament • Giving a priesthood blessing • Lessons from church on repentance and law of chastity • Anxiety of getting canceled |
| 3 | • Reading patriarchal blessing—idea that I have disqualified myself for the blessings promised • Romantic social situations overthinking romantic relationship: constant replay in mind • Platonic relationship situation of overthinking |
| 4 | • Going to the temple • Performing a live baptism • Accidentally referencing the temple in casual conversation |
| 5 | • Remembering past transgressions |
| 6 | • Romantic relationships/ • Anticipating getting sealed in the temple someday • Academic perfectionism |
| 7 | |
| 8–9 | |
| 10 |
You can see significant changes in his fear hierarchy near the end of his treatment process. In this chart nothing is ranked higher than a 6, and triggers were generally less frequent than they were at the beginning of treatment. He was particularly doing better with his academic perfectionism, claiming a much healthier mindset concerning it, but chose to rate it a 6 simply because as a university student the academic content was a daily presence in his life. As we evaluated his progress with this new fear hierarchy, it emphasized for us the work that still needed to be done, particularly in creating therapeutic exercises around the other items ranked as a 6. Near the end of his treatment process, he reflected on his therapeutic journey:
I began the recovery process while on my mission. I was able to call my family each Monday. Every call would end in sobbing, reassurance seeking, and increased anxiety because of my scrupulous tendencies. My selfless and loving parents would email me their love, advice for mental health, and articles on anxiety/
OCD throughout the week. I did not believe I had a diagnosable mental health condition until my mother sent me an article on scrupulosity. As I read the article, I sobbed because I had finally found what I was experiencing. The rest of my mission was far from easy. Luckily, I was able to start OCD medication on my mission, and I met with a therapist for a brief time on my mission until I was able to function. Though I could function, I struggled every day with feelings of unworthiness, guilt, and suicidality.
I was miraculously blessed with the opportunity to work with Dr. McClendon once I returned home. Attending therapy drastically improved my quality of life within weeks. I learned skills to regain control of my life and mental health.
An important part of my recovery was understanding that spiritual actions cannot mend a mental health condition. This was crucial to overcoming my scrupulosity. I learned I must take intentional and deliberate actions to improve my mental health.
Further, the cognitive skills and formal exposure techniques gave me clear action items to regain control of my mental health. I love the thought charts. These charts help ingrain healthy cognitive processes that breathe flexibility and contentment into my life.
I now know more than ever that God is my loving Heavenly Father, Jesus Christ is my Redeemer and Advocate with the Father, and the Holy Ghost is my companion of peace, love, and health. My scrupulosity did not bring me closer to God. The intentional and deliberate actions that I took in response to my scrupulosity brought me closer to God than I could have ever imagined. This life is a time to learn, progress, and love with greater health, fervor, and mercy.
Further, I found that I often adopted dogmatic and overly simple perspectives because I believed they would support my agenda. But in reality, the opposite is true. The more informed and nuanced my perspectives, the better I now understand myself, my community, and my humanity.
Example 3. The third client example is a college-age female, presenting to therapy for OCD treatment with a mixed presentation (several forms of OCD); she struggled with scrupulosity, self-harm, and sexual orientation OCD themes. I consulted with her and her parents while she was serving as a missionary. She made the difficult decision that, due to the complexity of her difficulties, it was best to return home to pursue OCD treatment.
While serving my mission for The Church of Jesus Christ of Latter-day Saints, and around the time of general conference, I began to have thoughts where I asked myself if I had enough faith. I questioned myself over and over again. I read and listened to a talk by President Nelson titled “Christ Is Risen; Faith in Him Will Move Mountains” over and over again as I got ready for my day. One of my companions actually called this compulsive behavior out as she was concerned for my well-being. I tried to redefine faith and what it actually meant, but for some reason my faith didn’t seem to be increasing and my thoughts of being unfaithful wouldn’t go away. No matter how much I read the scriptures and no matter how well I understood the doctrine, and how obedient I was being, these thoughts of faith didn’t cease. I repeatedly shared these concerns with my parents, companions, and mission president. Of course, they all reassured me and told me that what I was experiencing was normal and that increasing study of the gospel and changing my expectations would help. Nothing helped. For maybe a day or a few short hours, my constant guilt of not believing in the things I professed to believe would go away, but my disturbing thoughts only increased.
I soon found myself questioning every belief that I had ever had. Did I even believe anything? Did I know that the church was true? Would I be an active member of the church later? Was Jesus Christ my Savior? Is there a God? Did I believe everything that I was teaching people every hour of every day? Did I understand the difference between right and wrong? My entire world was flipped upside down and I couldn’t think my way out of it. The more I thought, the more I struggled. At times, I attributed it to homesickness, and although my mind kept telling me that I just needed to increase my gospel study and immersion in the mission, I soon came to realize that this was more than homesickness. I would often be on the verge of tears as I thought of what these thoughts and feelings would mean for me and my future. My mind was constantly caught up in these thoughts. I tried to push them away while teaching lessons or interacting with people, but they would still creep in. I literally became depressed and felt like there was no escaping the darkness that was my mind.
I was always known as “happy (my name)” and one of my catchphrases was “choose joy.” Joy didn’t even feel like an option. How could it be when I was constantly telling myself that I didn’t believe in the things that brought me and my family so much joy in the past? Other disturbing thoughts about harming others or myself entered my mind and still won’t seem to stop. I began meeting with a mission therapist who at first did not think that I had OCD. She and I both did not see that I was acting compulsively. One day, I had a panic attack and it was made clear to me that I had been acting compulsively. I let the therapist know and we began meeting more regularly. She had me expose myself to my thoughts that made me anxious. I would sit in the uncertainty for ten minutes. Oftentimes these exposures would drive me to tears, and the more anxious I was before the exposure, the more intense the sadness. This seemed to help for about a week, and I was able to see glimpses of happiness. However, my OCD or “scrup” (as I lovingly nicknamed it) came back with a vengeance. I kept working on exposures consistently, and it became apparent to me that the mission field was not the best place for me to figure out how to cope with my OCD and scrupulosity. It was difficult to discern what was a genuine thought and what was not. Everything became a trigger for me: seeing people living the gospel or people not living the gospel especially. Everything became a moral dilemma.
I believe that my stuck point was thinking about whether or not I will be an active member of the church later on. I think that is what all of my thoughts eventually stemmed from.
I felt frustrated. It was hard for me to realize that I decided to devote my life to sharing the gospel with people for eighteen months and that that was exactly what was hurting me so badly. Reading the scriptures and listening to conference talks also brought me a lot of anxiety. Subjectively, it would make sense that I could just choose what to believe, but everything I wanted to believe seemed to bring me anxiety. I just wished so badly that I could control my thoughts and choose what I wanted to believe and not let my thoughts attack me constantly. I felt like oftentimes I lived in fear and that I lived for distraction. Sometimes I felt hopeless. In the midst of my struggle, I just wanted relief and happiness. Not momentary, but lasting.
Her main fears were around scrupulosity and self-harm. You can see in table 14.8 how she completed her fear hierarchy.
Table 14.8. Client example 3: Fear hierarchy
| SUDs | Triggering Situation |
| 1 | |
| 2 | |
| 3 | |
| 4–6 | • Thoughts about the mission |
| 6 | • Thoughts about harming others • Thoughts about church doctrine • Thoughts about church structure |
| 7 | • Thoughts about self-harm • Being in public, concerts, shopping, etc.—places where I see people not living the gospel (e.g., smoking) • Social media • Having OCD thoughts about my OCD |
| 8 | • Going to church |
| 8½ | • Homosexual thoughts • Doubting God |
| 9 | • Thinking about my beliefs |
| 10 |
Figure 14.9 shows you her treatment outcome assessment data.
Figure 14.9. Client example 3: Outcome measures (OQ-45.2, PIOS-R, and Y-BOCS)
Three outcome measures track this client’s treatment progress: the OQ-45.2, the PIOS-R, and the Y-BOCS. As you look at the x-axis, you will see that this chart represents the first twenty-one sessions of her treatment. The first thing you can notice here is that, with an initial OQ-45.2 score of 64, this client is just one point above the clinical cutoff. She was functioning pretty well in general, but the pressure from the OCD was pushing up her distress. Second, take note on the y-axis that the clinical cutoff score for the PIOS-R is 24 and this client’s initial score on the PIOS-R was 39. Based on my clinical experience, I would consider this a moderately high level of scrupulosity.[26] Third, the client also was administered the Y-BOCS. Her initial Y-BOCS score for session one, seen along the y-axis, was a 22. According to Y-BOCS researchers, a 22 represents a moderate level of clinical OCD disturbance.[27]
As you examine this chart representing the outcome measure scores for this client, you can see that her OQ-45.2 scores and her Y-BOCS scores shifted up and down a bit over the first fifteen sessions, although the PIOS-R continued steady decline throughout the therapy process. This is particularly significant, considering scrupulosity was not our only focus during treatment. Up to half of her exposure time was also spent on self-harm exposures, yet the impact of treatment on her scrupulosity is strong. Treatment was weekly, then went to every other week, and then went to once a month. We continued to meet once per month for some time to stabilize and maintain treatment gains—her scores continued to drop even further! Her final OQ-45.2 score on this chart is a 31, solidly below the average, normal range (a score of 45 is average for a community sample). The final PIOS-R score on this chart is a 14, well under the clinical cutoff of 24 (meaning that her scrupulous fears were no longer causing significant interference in her life). And her the final Y-BOCS score on this chart was a 10, which represents a mild OCD severity score.[28]
After thirty sessions, we adjusted her hierarchy of fears to reflect the improvements she had made in therapy and to highlight for us the areas that still needed more attention. See table 14.10.
Table 14.10. Client example 3: Client’s adjusted fear hierarchy
| SUDs | Triggering Situation |
| 1 | • Being in public, concerts, shopping, etc.—places where I see people not living the gospel |
| 2 | • Thoughts about harming others |
| 3 | • Thoughts about church doctrine • Thoughts about church structure • Social media • Having OCD thoughts about my OCD • Going to church |
| 4 | • Thoughts about the mission |
| 5 | |
| 6 | • Thoughts about self-harm • Homosexual thoughts • Doubting God |
| 7 | • Thinking about my beliefs |
| 8 | |
| 9 | |
| 10 |
As you can see, her fears shifted down quite a bit. Going out in public used to be a 7 and it was now a 1! She said she wouldn’t even consider seeing someone smoking as any kind of anxiety trigger for her scrupulosity at this point. This was a huge victory for her because it had gotten very difficult for her to go anywhere without her anxiety getting triggered by everything she saw: “Maybe I want to do that, too?”
Her greatest fear, “Thinking about my beliefs,” shifted from a 9 to a 7. This trigger, holding steady at a 7, highlighted for us the need to spend more time on it explicitly in therapy, since her priorities had been other exposures centering on scrupulosity and self-harm. Yet even though a shift from a 9 to a 7 perhaps doesn’t seem like much, that change represents a huge qualitative change in her quality of life. A 9 is intense and represents a very poor quality of life. She said: “For me, a seven is not crying, but nine is crying. That’s how I judge it. I would have a constant feeling in my throat of crying, always trying to hold it in—and I’m not a crier, so that’s something. But now I don’t feel that way anymore.”
Near the end of her treatment process, she commented:
I started on the road to recovery by recognizing that something was wrong and that I wanted to fix it. My world had literally flipped upside down and I couldn’t comprehend who I was. I talked to my extremely supportive parents about my struggles, and they went to work on finding me help. Once I found a therapist, I went to work on therapy homework. Making progress with OCD takes persistence and consistency. I decided that I would work hard so that I could be myself again.
The most important thing in my recovery was hope. It was extremely hard for me to find hope for months. I felt like I would never see the light, and I felt uncomfortable being with my thoughts. I genuinely hated being in my own skin. Somehow I found hope in persistence. Because I was working toward recovery, I found purpose. I wanted to find the sunshine in my life again, and I knew that steady effort was the only way to find that.
Scrupulosity dug into every part of my life, and honestly it was hard to find purpose. I’ve found meaning because I get to choose how I live my life. I’m not controlled by my anxiety and scrupulosity. I get to be myself and do things I enjoy. There were small victories along the way that reminded me who I was. For example, attending church was difficult for me because of my scrupulosity. I remember thinking one Sunday that it wasn’t as hard as it used to be. That victory and others propelled me forward to do exposures and other therapy homework. I found that hope takes action.
OCD is no joke. It is genuinely the hardest thing I’ve experienced. . . . I still struggle with my OCD, and I’m learning to accept the implications it has in my life, but my life experience is worlds away from what it was in the depths of my struggle.
After her recovery, this client summarized that the biggest changes for her were being able to be present in her life without having to think about other things and being able to feel happiness. One item on the OQ-45.2 questionnaire asks for a response to the statement “I am a happy person.” This client began to cry when she recognized that after marking her answer as “Rarely” for this statement at the beginning of her therapy process, she was now able to answer: “Almost Always!”
Example 4. While some therapeutic changes occur over time, some happen more quickly. One woman, a cancer-survivor and widow in her late sixties, traveled to my state of Utah to do a “crash course” therapy process. We met for two to four hours each day, for a total of twenty-two sessions over a week and a half. Before beginning therapy she shared part of her story:
I always felt guilty over little things as a child and was a “rule follower” and I would worry a LOT. I had extreme awareness of people in positions of authority: teachers, doctors, clergy, policemen, and the school principal. I often was afraid of people in authority, and that I’d do something wrong, but I wasn’t a bad kid. Once I got a ticket for riding my bike on a downtown sidewalk and had go to traffic school (for kids). That haunted me for years!!
Gradually I felt more responsible and felt I should take blame, or had the need to confess minor things. OCD began with just a “something’s wrong/
not right” feeling. Then in college it took on more of a moral or religious meaning and on and off into adulthood. It seems to be at its worst in the last few years, as I’m alone with my thoughts. My “stuck point” is that now the “action precedes the thought.” Certain actions (shutting doors, walking over lines, preparing food, driving over speed bumps—basically things everyone encounters every day) trigger the unacceptable thoughts about respected leaders, and I have to repeat the action until I can do it without thinking the bad thought (which I find very blasphemous and offensive). If not, I’ve offended God for not “repenting” (fixing, do-over) and something very bad could happen—a leader could die and it would be my fault. But after, I feel angry (and foolish) at myself for “giving in” to the ritual.
I loathe the thoughts, and I know I don’t really mean or want them. I think it’s disgusting. It’s not part of my belief system or “who I am,” and when it happens I feel weak, angry, and frustrated, and I often yell. I’m so mad that I’ve allowed this insane OCD to “win,” but I HAVE to “fix it” until I feel better.
Writing this down in print is really hard and embarrassing. I’m afraid I don’t really have OCD—that I’m just insane or a very bad person.
She had many fears about things needing to be made “right” and needing to retrace. Her biggest fear involved frightening thoughts about respected leaders. You can see in table 14.11 how she completed her fear hierarchy.
Table 14.11. Client example 4: Fear hierarchy
| SUDs | Triggering Situation |
| 1 | |
| 2 | |
| 3 | • Getting dressed, including jewelry |
| 4 | |
| 5 | • Knitting (repeat stitch) • Piano playing (repeat measures of music) |
| 6 | • TV with remote (going back, deleting watched programs on DVR) |
| 7 | • Crossing lines or shadows while walking or driving • Kindle reading—retapping page turn repeatedly • Writing (needing to retrace and erase letters and words) |
| 8–9 | • Thresholds, using keys, closing doors, cabinet drawers • Printer (if have “bad” thought when hit the print button have to throw away copy that is made) |
| 10 | • Fears of harm befalling any respected leader because of any thought (even a benign thought) while doing any of the above. • Food restrictions |
Figure 14.12 shows you her treatment outcome assessment data.
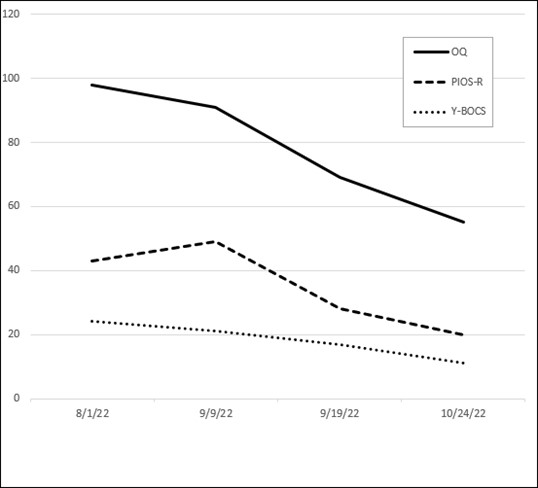
Figure 14.12. Client example 4: Outcome measures (OQ-45.2, PIOS-R, and Y-BOCS)
Description of scores. Three outcome measures tracks this client’s treatment progress: the OQ-45.2, the PIOS-R, and the Y-BOCS. As you look at the x-axis, you will see that this chart shows only four data points due to the nature of her treatment process. The first two data points were both baseline scores. The first was taken five weeks before meeting, while the second was taken the day we started treatment. The two baseline scores established that her high level of distress was consistent prior to treatment.
The first thing you can notice here is that, with initial OQ-45.2 scores of 98 and 91, this client was in high distress (the clinical cutoff score is 63). She was not functioning well with OCD pressing into every area of her life. Second, take note on the y-axis that the clinical cutoff score for the PIOS-R is 24 and this client’s initial scores on the PIOS-R were 43 and then 49. Based on my clinical experience, I would consider this a severely high level of scrupulosity.[29] Third, the client also was administered the Y-BOCS. Her initial baseline Y-BOCS score, seen along the y-axis, was 24, while the second baseline score was 21. According to Y-BOCS researchers, a 24 is severe while a 21 represents a moderate level of clinical OCD disturbance.[30]
Please note that there are only ten days between the second and third data points, showing a rapid decrease in distress due to the intensive treatment intervention. As you examine the third and fourth data points, representing the outcome measure scores for this client, you can see that her OQ-45.2 scores, PIOS-R scores, and her Y-BOCS scores all dropped significantly during the week and a half of intensive treatment (to 69, 28, and 17 respectively) and continued to drop after treatment as she continued to practice at home what she had learned in treatment (to 55, 20, and 11 respectively; the follow-up scores were obtained five weeks after treatment). The follow-up scores (the fourth data point) show her solidly in the average, normal range for the OQ-45.2 and the PIOS-R (a score of 45 is average for a community sample for the OQ-45.2, and the clinical cutoff for the PIOS-R is 24). And the fourth Y-BOCS score on this chart was 11, which represents a mild OCD severity score.[31] Almost three months later, she traveled to Utah again for a family event, so we met for a follow-up appointment. Before this meeting, she filled out the questionnaires again. This time her OQ-45.2 was 56 (within the normal range), her PIOS-R score was 22 (below the clinical cut-off of twenty-four), and her Y-BOCS score was 14, a mild score. These scores are only slightly up from the scores almost three months earlier, showing that she was doing well maintaining her therapy gains. After beginning treatment in severely high distress, she was now functioning very well, with only mild OCD interference.
When she took her follow-up questionnaires five weeks after completing her crash course in therapy, she also adjusted her hierarchy of fears to reflect the improvements she had made in therapy—and was still making—as she continued to work the therapy process. See table 14.10.
Table 14.13. Client example 4: Client’s adjusted fear hierarchy
| SUDs | Triggering Situation |
| 1 | • Getting dressed, including jewelry • Piano playing (repeat measures of music) |
| 2 | • Knitting (repeat stitch) • Writing (needing to retrace and erase letters and words) • Printer (if have “bad” thought when hit the print button have to throw away copy that is made) |
| 3 | • Kindle reading—retapping page turn repeatedly • TV with remote (going back, deleting watched programs on DVR) • Crossing lines or shadows while walking or driving • Thresholds, closing doors, cabinet drawers |
| 4 | • Using keys • Food restrictions |
| 5 | • Fears of harm befalling any respected leader because of any thought (even a benign thought) while doing any of the above. |
| 6 | |
| 7 | |
| 8–9 | |
| 10 |
As you can see, she had experienced significant, life-changing improvements to her distress! Every fear had dropped significantly, so even her worst, most terrifying fears were now only rated a 5. Five weeks after ending her “crash course” treatment process, she wrote about getting into treatment, as well as her journey through treatment:
I was utterly exhausted and could not see the rest of my life in this endless cycle of what I knew was a ridiculous, senseless, illogical, and unhealthy way of living. I didn’t feel God wanted this for me either. I had researched and read enough about OCD to know what I needed to do, but lacked the courage and was fearful to “take the leap.”
I had prayed (a lot) about my “issues” and stumbled onto an article written by a therapist of my faith (this was important to me). After watching her online OCD course, and crying through the entire thing, I felt I had some questions—personal to my situation and thoughts—for which I needed to seek answers in person. Gratefully, she arranged to see me. At this point, I felt this was my “last chance” to end the relentless monotony or just give up and continue on in the same way.
With the decision to get counseling, I committed to the treatment with full honesty and transparency in our sessions (as embarrassed as I was revealing the “craziness”). I gave dedicated time and effort to the assignments and to what I needed to do to get the most from this help. I am still not totally “cured,” but I am much improved. I continue to work on and face exposures daily (and it’s still sometimes hard), review notes from therapy, rewatch the online course, and read recommended literature.
There was a combination of several things involving psychotherapy that contributed to beginning my recovery. First was my prayerful dedication and commitment to accept the formal psychotherapy treatments as basic and sound truth. This was everything. Next, I desperately needed to trust my therapist so I could believe and accept her reassurances that she understood my symptoms and fears, and, most importantly, KNEW ME—my “real self,” my personality, my values, and my struggle with OCD. It was important to hear I was not insane, or worse, evil, and that OCD and scrupulosity were “real disorders.” I could then allow myself to “transfer the inflated responsibility for my guilt.” I also came to the understanding that “My Faith was stronger than my OCD.” I was able to exercise faith where anxiety existed and let go of compulsions. Beneficially, I understood the Atonement more fully.
Moving forward as I continue to “work” on scrupulosity (and it is still ”work” at times), I feel so much more hope. I feel “lighter,” no longer dragged down mentally and emotionally by rituals and frustrations. Life is simpler and I feel more creative and happier. My brain isn’t so cluttered with time-draining “have to” repetitions. I feel unencumbered by meaningless details to “fix the thought.” It’s become “okay” to skip the cycle, even if it is a bit uncomfortable. It’s very freeing to be just plain me again!
She also wrote the following to me in an email full of light and hope:
I still occasionally have my “moments,” but I’m feeling SO much better, happier, and hopeful. It feels so good not to be weighed down and anxious all the time. You should see me bounce over those speed bumps! Most of the time, I’m so busy thinking “normal thoughts” I completely forget they are even there until after I hit them! The first time that happened, I laughed out loud and thought of you! I actually completely forgot it was coming! “I’ve got to tell her!”—only you would share the irony! Life is looking good.
Other Stories of Therapeutic Progress
One college-aged man with a severe level of scrupulosity initially rated attending the temple as his top fear on his fear hierarchy. He ranked doing temple baptisms as a 9 out of 10 and going to the temple to participate in an endowment session as a 10 out of 10. And then he ranked an 11 on his 10-point scale—going to the temple and doing an initiatory ordinance was for him an 11 out of 10! It was simply impossible for him. In addition to addressing his other scrupulous fears, we worked on his temple fears in therapy for quite some time. He made some progress, but we were legitimately handicapped because the temples were closed at that time due to the COVID-19 pandemic, so he could not physically go to the temple for in vivo exposures to expand our exposure work.
When the time came that the temples reopened, he began to go frequently to the temple for therapeutic practice. There was little spiritual uplift for him in those earlier sessions; attending was just an exposure exercise. However, after some time, going to the temple shifted for him. Instead of feeling like a therapeutic exposure exercise, it began to feel like “just going to the temple.” He then started to have good experiences in the temple. Near the end of his treatment process, full of light and peace, he shared some of his positive experiences and then said, causing tears to come to my eyes, that he had just met with his bishop to inquire about becoming a temple worker. Later, he reported to me that he had become a temple worker, volunteering there every week. Wow! After getting proper treatment for his OCD, the temple, which had been a source of agonizing, paralyzing fear, had now become a place of peace, a place that he desired to be, and he wanted to make it part of his lifestyle. He later commented: “Exposures are not fun, but they are necessary to break free from the crushing grip of OCD. When unobscured by anxiety, I find that the Gospel of Jesus Christ really is a beautiful message of hope, peace, forgiveness, mercy, grace, and redemption through Jesus Christ.”
Another individual commented on shifts she began to see some time into her treatment:
The first time I truly understood the “joy of repenting” was just a few months ago. Because of the benefits of exposure therapy, I had really started praying again and could feel my fear of living the gospel turning to faith. After a simple disagreement with my spouse, that budding faith encouraged me to pray for forgiveness. I lay in my bed and started to talk simply with Heavenly Father, asking for help and forgiveness. I was expecting similar feelings of guilt and shame. Instead, I started to feel peace and hope.
I paused—almost in shock—taking in the moment.
Was this the joy I’d heard about for so long?
The peaceful assurance that came confirmed it. For the first time, in a long time, I felt freed “from the enemy which had me bound.”[32]
Treatment benefits last long term, especially if you keep up a lifestyle of enacting therapeutic principles. One woman shared this about her therapeutic journey with scrupulosity:
Over the past 10+ years since that experience, through the Spirit, through trial and error, and with the help of more professional counseling, my understanding of what’s really true has become much more clear, and I’ve been able to feel differently about things in my life than I had in the past. I’ve come to feel the difference between the Spirit gently whispering to me when I have actually sinned and when a correction is needed vs. the relentless anxiety that led me to obsess about every tiny mistake and to try to be absolutely perfect in every detail. I’ve learned how to repent in a productive and cleansing way when I sin instead of the compulsive, repetitive, futile “repentance” I was driven to in the past.
As discussed in chapter 3, we all experience random intrusive thoughts, some of which are distasteful to us, even nasty, absolutely hideous thoughts. These unwanted thoughts will not miraculously disappear from your brain after successful OCD treatment. But the anxiety and the need to control those thoughts may be severely reduced, while the intensity and frequency of the thoughts will also likely decrease. This same woman continued to say this about her current relationship to her OCD: “As far as the OCD, I still have lingering tendencies towards details and honesty and exactness, but by being mindful of when these things creep in, I’ve come to a point where I can dismiss them quickly most of the time, even without the help of medication.” As she shows us here, some of this lingering is positive. You want to retain your conscientiousness, your devout love of God, your integrity, your loyalty, your attention to detail in doing a job well. The difference is one of degree and function.
One married man in his sixties recovered from scrupulosity many years ago. He explained the idea of lingering tendencies this way: “My loyalty to God and desire to be completely honest is still there. It was just necessary to recalibrate that loyalty in a healthy way. I believe I’m more loyal now than I’ve ever been; it’s just manifested in the correct and healthy actions and feelings. When those anxious moments start to move in, I shift toward giving myself the space to walk away from it for a day or two, then look at it again later through a proper perspective.” It is often the case that people fear that therapy is giving them a chance to rationalize or justify sin or to be led astray. That is not the case. You will retain your earnest devotion, yet it will become healthier. You’ll be free to continue to expand your relationship with Deity as you are ready to receive it. And that personal worship will be manifested in a way that allows for flexibility and wholeness.
One client, a married man in his twenties with two children, said this about his recovery:
Not only do I feel like I have come out as a whole person, but I also feel like I have discovered and learned valuable lessons about myself, mental health, and the gospel of Jesus Christ as scrupulosity, in my context, was closely connected to my faith. I feel far more compassionate now to those who suffer from mental health challenges, and I feel a sense of purpose in trying to help with those who suffer in this way. In addition to a greater level of empathy to those who suffer in mind, I also have acquired a healthier perspective on personal progression and what God expects of me. I used to be hyperfocused on perfecting myself, but I now feel a greater trust in God’s ability to do that for me. I am more comfortable with my weaknesses and can see how God’s grace is sufficient. My life after therapy has brought me more joy, a clearer understanding between what is the Spirit and what is my anxiety, an improved and closer relationship to God and my wife and an enhanced level of gratitude for living.
Some time after treatment with this client ended, I was able to follow up with his mother. She reported a stark contrast in her son since he had completed treatment: “overall—like a huge weight or burden has been lifted. He seems much more relaxed and at peace with the learning and growing process of life—much more able to be himself. He is openly grateful and joyous of the difference this therapy has made in his life, and the tools and understanding he feels like he now has to recognize and navigate situations that would’ve previously brought anxiety and distress.” Then she said: “I could also add that his whole concept of Heavenly Father changed.” As we heard from him, in his own words, that concept of God has changed for the better; he trusts God and understands the Atonement of Jesus Christ will cleanse and save him. He has reclaimed the ability to find joy and peace in his religious belief. I know that this is possible for each of you. It may be a difficult journey, and it may be a scary one, especially as exposure triggers your anxiety initially. And yet if you will hang in there and trust the therapy process, you can reclaim the relationship you want with the God whom you worship and love.
Seek Treatment If Needed or Desired
As you’ve worked your way through this book, you’ve learned a lot about scrupulosity. In these latter chapters on treatment, you’ve learned about principles of effective scrupulosity OCD treatment, and perhaps you’ve begun to implement some of these principles with their accompanying exercises into your life. I’ve presented principles to help you build a healthy emotional foundation: self-soothing, meditation, TIP skills, and building positive-sentiment activities into your life. I’ve discussed the cognitive domain, identified distortions, and introduced you to some cognitive techniques. Perhaps you’ve already started identifying your distortions, labeling them for what they are, and recognizing that the anxiety is lying. Perhaps you’ve challenged your distortions and you’ve even worked through them to try to find more reality-based thoughts through thought charts or other cognitive methods. Maybe you’ve worked on exposures. Maybe the first few were a bit rough, but maybe now you’re getting the hang of how the process works and building some confidence in your ability to do them. Keep working the process; the self-help format can be helpful. A case study of a married twenty-three-year-old Muslim man with scrupulosity, suffering with obsessional blasphemous thoughts and sexual images of the divine, found that a self-help format of a cognitive program with ERP was effective at decreasing his obsessive-compulsive symptoms and decreasing toxic guilt.[33]
Yet maybe something isn’t clicking for you. Maybe you’ve gone back through these treatment chapters a few times and have been working diligently on implementing these treatment principles, but you feel you are just not making the therapeutic progress you desire. I have included some additional self-help treatment resources for you in appendix 6. However, please don’t give up if the self-help format is not working for you as well as you hoped. If you need help or additional support facing the top fears on your fear hierarchy, please don’t hesitate to solicit the help of a mental health professional. Elder Alexander B. Morrison taught: “Just as we would not hesitate to consult a physician about medical problems, such as cancer, heart disease or diabetes, so too we should not hesitate to obtain medical and other professional, appropriate professional assistance in dealing with mental illness.”[34] Indeed, research has shown that therapist-assisted exposure is more effective than patient-directed exposure.[35] The mental health professional can assist you to personalize the OCD treatment to best fit your unique needs and circumstances.
I would encourage you to seek help from a competent psychologist, or other mental health professional, that is trained in the treatment of obsessive-compulsive disorder. Preferably your mental health professional would understand scrupulosity and have treated it previously. However, a mental health professional who has worked with OCD but has not previously treated someone with scrupulosity may still be useful to you since treatment can be modified to better fit scrupulosity.
Conclusion
There is hope! You can change your life! One client offered this encouragement: “If you really want a stronger, closer connection with God and be able to hear his voice more clearly, then make therapy a priority because therapy helps clear out the chaos that disrupts your relationship to God.” Indeed, you can quiet anxiety’s harsh accusations and find hope and healing. You can experience the comfort, joy, and peace that you desire while embracing your most deeply loved and cherished beliefs.
Thank you for journeying through Freedom from Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD. I wish the very best to you on your continued journey toward health and happiness!
Notes
[1] Abramowitz, J. S., & Arch, J. J. (2014). Strategies for improving long-term outcomes in cognitive behavioral therapy for obsessive-compulsive disorder: Insights from learning theory. Cognitive and Behavioral Practice, 21(1), 21. https://
[2] McLeod, S. A. (2019, July 10). What does effect size tell you? Simply Psychology. https://
[3] Olatunji, B. O., Davis, M. L., Powers, M. B., & Smits, J. A. J. (2013). Cognitive-behavioral therapy for obsessive-compulsive disorder: A meta-analysis of treatment outcome and moderators. Journal of Psychiatric Research, 47(1), 35. https://
[4] Abramowitz, J. S. (1997). Effectiveness of psychological and pharmacological treatments for obsessive-compulsive disorder: A quantitative review. Journal of Consulting and Clinical Psychology, 65(1), 44–52. https://
[5] Kobak, K. A., Greist, J. H., Jefferson, J. W., et al. (1998). Behavioral versus pharmacological treatments of obsessive compulsive disorder: a meta-analysis. Psychopharmacology, 136(3), 205–216. https://
[6] Eddy, K. T., Dutra, L., Bradley, R., & Westen, D. (2004). A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clinical Psychology Review, 24(8), 1011–1030. https://
[7] Rosa-Alcázar, A. I., Sánchez-Meca, J., Gómez-Conesa, A., & Marín-Martínez, F. (2008). Psychological treatment of obsessive-compulsive disorder: A meta-analysis. Clinical Psychology Review, 28(8), 1310–1325. https://
[8] Abramowitz, J. S., Franklin, M. E., & Foa, E. B. (2002). Empirical status of cognitive-behavioral therapy for obsessive-compulsive disorder: A meta-analytic review. Romanian Journal of Cognitive & Behavioral Psychotherapies, 2, 89−104.
[9] Abramowitz, Franklin, & Foa, 2002. Empirical status of cognitive-behavioral therapy for obsessive-compulsive disorder, 89−104.
[10] Franklin, M. E., & Foa, E. B. (1998). Cognitive-behavioral treatments for obsessive-compulsive disorder. In J. M. Gorman (Ed.), A guide to treatments that work (pp. 339–357). Oxford University Press.
[11] Keeley, M. L., Storch, E. A., Merlo, L. J., & Geffken, G. R. (2008). Clinical predictors of response to cognitive-behavioral therapy for obsessive-compulsive disorder. Clinical Psychology Review, 28(1), 119. https://
[12] Rufer, M., Fricke, S., Moritz, S., etal. (2005). Symptom dimensions in obsessive-compulsive disorder: Prediction of cognitive-behavior therapy outcome. Acta Psychiatrica Scandinavica,113(5), 440–446. https://
[13] Starcevic, V., & Brakoulias, V. (2008). Symptom subtypes of obsessive-compulsive disorder: Are they relevant for treatment? Australian & New Zealand Journal of Psychiatry, 42(8), 651–661. https://
[14] Olatunji, Davis, Powers, & Smits, 2013. Cognitive-behavioral therapy for obsessive-compulsive disorder, 35.
[15] Keeley, Storch, Merlo, & Geffken, 2008. Clinical predictors of response to cognitive-behavioral therapy for obsessive-compulsive disorder, 120.
[16] Keeley, Storch, Merlo, & Geffken, 2008. Clinical predictors of response to cognitive-behavioral therapy for obsessive-compulsive disorder, 120.
[17] Keeley, Storch, Merlo, & Geffken, 2008. Clinical predictors of response to cognitive-behavioral therapy for obsessive-compulsive disorder, 126.
[18] Olatunji, Davis, Powers, & Smits, 2013. Cognitive-behavioral therapy for obsessive-compulsive disorder, 39.
[19] Lambert, M. J., & Ogles, B. M. (2004). The efficacy and effectiveness of psychotherapy. In M. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior change (5th ed.). Wiley, 156.
[20] Buchholz, J. L., Abramowitz, J. S., Blakey, S. M., et al. (2019). Sudden gains: How important are they during exposure and response prevention for obsessive-compulsive disorder? Behavior Therapy, 50(3), 678.
[21] Shapiro, L. J., Krompinger, J. W., Gironda, C. M, & Elias, J. A. (2013). Development of a scrupulosity severity scale using the Pennsylvania Inventory of Scrupulosity-Revised. Journal of Obsessive-Compulsive and Related Disorders, 2, 420–424. https://
[22] According to L. Shapiro (personal communication on August 19, 2019), a score of 42 would be in the severe range.
[23] See note 22.
[24] Goodman, W. K., Price, L. H., Rasmussen, S. A., et al. (1989). The Yale-Brown Obsessive Compulsive Scale: I. Development, use, and reliability. Archives of General Psychiatry, 46(11), 1006–1011. https://
[25] Goodman, Price, Rasmussen, etal., 1989. The Yale-Brown Obsessive Compulsive Scale, 1006–1011.
[26] See note 22.
[27] Goodman, Price, Rasmussen, et al., 1989. The Yale-Brown Obsessive Compulsive Scale, 1006–1011.
[28] Goodman, Price, Rasmussen, et al., 1989. The Yale-Brown Obsessive Compulsive Scale, 1006–1011.
[29] See note 22.
[30] Goodman, Price, Rasmussen, et al., 1989. The Yale-Brown Obsessive Compulsive Scale, 1006–1011.
[31] Goodman, Price, Rasmussen, et al., 1989. The Yale-Brown Obsessive Compulsive Scale, 1006–1011.
[32] Vogrinec, W. (2021, March 2). OCD, God, and me: One woman’s experience with scrupulosity. LDS Living. https://
[33] Choudhary, V., Bose, S., & Sharma, P., & Ghimire, S. (2016). ERP with cognitive bio-behavioral self treatment in blasphemous OCD: A case report. International Journal of Analytical, Pharmaceutical and Biomedical Science, 5, 9–12.
[34] Morrison, A. B. (2005). Myths of mental illness. Ensign, 33–34. https://
[35] Abramowitz, J. S. (1996). Variants in exposure and response prevention in the treatment of obsessive-compulsive disorder: A meta-analysis. Behavior Therapy, 27(4), 583–600. https://
