Self-Help Treatment
Specific Exposure Exercises
Debra Theobald McClendon, "Self-Help Treatment: Specific Exposure Exercises," in Freedom From Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Provo, UT: Religious Studies Center, Brigham Young University; Salt Lake City: Deseret Book), 249–82.
Preparing for Exposure
Motivation to engage in exposure and response prevention (ERP)
ERP can be scary. Admittedly this is by design, as the therapeutic exercises need to push your comfort zone and activate your fear network to be effective in diminishing anxiety. If you are feeling hesitant to begin, consider engaging in some of the specific cognitive exercises presented in chapter 11. You can try a cost-benefit analysis, which is by nature a motivational technique. You can list all the advantages to continuing to resist engaging in the exposure process against all the disadvantages for doing so. A thought chart could also be particularly helpful here. Try putting into row A the statement “Preparing to do my first exposure session for therapy.” What fears come up for you? Put those in row B. Then work the thought chart from there.
Also, you may need to simply keep in mind that the pain of exposure is temporary, while the pain of not doing exposure is long-term. How long have you already suffered with scrupulosity? How much longer are you willing to suffer before engaging in the gold-standard treatment?
One client, a single woman in her early twenties, acknowledged and honored the difficulty of exposures by not only tracking her Subjective Units of Distress Scale ratings (SUDs; how high her distress was through an exposure) but by keeping track of her “Tissue Scale” (how many tissues she used during the exposures due to the difficulty of the exposures bringing her to tears). She found that exposures got much easier with time. Several months into her therapy process she reported that she was less afraid to do her exposures, that they had become part of her routine: “I’m just going to do them, and they will help me. That is the biggest difference. I’m not so afraid to do them. During the exposures now they are also not as difficult—not as many tissues.”
Another client, a single woman in her thirties, reflected on her therapy journey. Even though she was still fairly new to exposure, she was beginning to see therapeutic progress, which gave her hope. She indicated that the entire OCD experience—which for her included not only the therapy work but also trying medication—was a huge test of faith. Even while recognizing she had more work to do therapeutically, she reported feeling happier in general. “I see the blessings of testing and pushing and putting the work in. I’m happy to see differences in myself, and other people can also see differences in myself. Just seeing progress makes me happy.”
Accepting the risk of sin
Exposures may trigger your fear that you are advocating sin or accepting sin into your life. Instead, during exposure you accept the risk of sin. Your trigger “sins” are generally things the OCD has mislabeled as sinful but are not. In accepting the risk of sin during an exposure, you should not knowingly or blatantly choose sin, or follow any mental health professionals if they encourage you to do so. Encountering risk of sin causes anxiety (which we do want to provoke in exposure treatment of scrupulosity); if it doesn’t feel risky to you it won’t provoke anxiety nor be an effective intervention. However, legitimate sin provokes guilt in a religious believer, not anxiety. A researcher has clarified this caveat:
Instructions to flagrantly violate religious laws are neither appropriate nor necessary to reduce pathological fears of sin. Patients with scrupulosity fear they might have sinned. Therefore, exposure should entail situations in which there is only the risk of sin—yet enough of a risk to evoke the patient’s uncertainty.[1]
Other researchers have echoed emphatically against having religious clients accept sin as part of treatment. They believe that if a client’s religious community views a belief or act as sinful, the person should not do it.[2] Please don’t go out and sin and call it an exposure. That’s not an exposure. You are seeking to be exposed to the fears that are triggered by your deep core fears. And the fear of the possibility of sin—expressed in the plaguing question “What if I’ve sinned?”—needs to be triggered by these exposures. You and your mental health professional need to “work within the limits of religious practice.”[3]
If you need additional help making these nuanced distinctions, authors have suggested using a spiritual advisor, someone who has the same religious beliefs and a basic understanding of OCD and scrupulosity. This does not need to be an ecclesiastical authority, but could be a friend or family member. You can then explain your proposed exposure tasks to your advisor and ask the question, “Is this morally acceptable to do?” You can adjust the tasks until you feel the therapeutic tasks are acceptable to both you and your advisor.[4]
So what would accepting the risk of sin look like during an exposure? Exposure practices involve deliberately behaving in ways you misunderstand to be “amoral, sinful, and worthy of punishment from God, but that really [are] not such infractions.”[5] It is not necessary or of value to tell yourself you are sinning while doing exposure. Generally, using a simple exposure statement maximizing uncertainty will be sufficient, such as “Maybe I’m sinning, maybe I’m not. It’s hard to tell” or “I’m not sure if this is sinful. It could be, but I’m doing it anyway.”
As seen in these exposure statement examples, you can emphasize this type of uncertainty by including “uncertain” terminology, with as many variations as possible, in your exposure work. You can include uncertainty in your formal exposures or use them as stand-alone exposures when you encounter a naturally occurring anxiety trigger in your daily activities. Many clients default to using “Maybe” or “Maybe [this] . . . maybe [that]. I don’t know.” This is effective, but there are also many more available options to elicit a feeling of uncertainty. (The longer phrases in the bottom third of the “I Am ‘Uncertain’” list in the sidebar can be added to the end of any of the sentence starters in the top two-thirds of the list for heightened uncertainty.)
With this emphasis on the uncertainty of sin during exposure, you face the possibility of your feared consequence without it actually occurring.[6] This is no easy task. One client stated that she was “petrified of the uncertainty.”
For example, scrupulous clients with obsessions about possible inappropriate sexual touching of their children (which in their anxious minds would mean they had sexually abused their children, and this would lead to a whole host of other extreme, dreaded, legal, familial, and religious consequences) tend to have significant difficulty interacting with, bathing, and holding their young children. If this is part of your experience, an effective exposure process may be to select exposures that tend to happen already during daily living but that perhaps you have highly restricted or now completely avoid due to your scrupulous anxiety. Several clients chose to repeatedly wrestle playfully with their children. Another client chose to repeatedly hold several of her small children on her lap at the same time while reading to them. In both exposure conditions, body parts of both the adult clients and their young children were getting squished and bumped up against each other, or children were grabbing body parts to help them hold on to the parent. Although the initial exposures produced high levels of anxiety, as the exposures continued, anxiety decreased and the clients were able to physically interact with their children more freely. This had a significant positive influence on their relationship overall. One of these clients, nearing the end of his treatment, commented that the wrestling had gotten to the point that he didn’t even notice he was doing it as an exposure—but that he was doing it just because he wants to play with his kids. What a tremendous, freeing milestone!
Consultation with religious authority
If you are not able to resolve concerns you may have engaging in exposures for OCD treatment, clergy involvement can be helpful (and may even be essential). Researchers suggest that you may have your mental health professional (if you are working with one) engage in direct discussion with your ecclesiastical leader. This meeting would generally have goals of coming to mutual understanding about the therapy process, creating an atmosphere of collaboration, and reducing your suffering. Advances in technology make this practical today, as you, the therapist, and the clergy member can generally all participate in the meeting, such as over speakerphone or video chat during a therapy session.[7] More informally, it can also be helpful to have your ecclesiastical leader and mental health professional converse over the phone.
If you are uncomfortable with direct contact between your therapist and ecclesiastical leader, or if it is not feasible to do so, then you can meet directly with your clergy member to discuss your concerns. If you take this approach, researchers suggest it would be most effective to prepare with your therapist by creating questions that will be asked of the ecclesiastical leader. This preparation can help you avoid the potential for rituals or reassurance seeking. Researchers also recommend that you should record your discussion with the church leader to minimize post hoc rationalizations or obsessive uncertainty.[8] If you record your discussion with your church leader, you can listen to it with your therapist. A recording would be helpful to allow your therapist to clarify anything you may have misunderstood from the discussion.
Hierarchy of fears[9]
How do you know where to start with your first exposure? First, construct a hierarchy of fears. Different fears trigger your anxiety at different levels. So create a hierarchy, ranking the things that trigger your anxiety in a list format. Make a list of the numbers one through ten (or one to one hundred, if you prefer), then jot down fears or anxiety-triggering stimuli next to the corresponding number. Some numbers may not have anything filled in next to them, and other numbers may have multiple fear items. You’re just going to record what is true for you.
Let’s look at a few examples of a hierarchy of fears constructed by clients struggling with scrupulosity to give you a good idea of what this will look like. The first client’s main concerns centered around fear of sin and sexuality. The second client’s fears focused on sexual arousal, particularly fear about being a pedophile and abusing his children. The third client’s fears centered around self-harm and religious doctrinal fears.
Table 13.1. Fear hierarchy example 1[10]
| SUDs | Triggering Situation |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | • I can’t recall every sin, so every sin will not have been “properly” confessed. |
| 6 | |
| 7 | • Sins I can remember: Did I confess? And did I confess properly? • Is my desire to fight scrupulosity just an effort to rationalize sinful behavior? |
| 8 | • Sexual thoughts popping up. • Is this wish fulfillment? Did I really want to . . .? • Going on a date. |
| 9 | • Sexual thoughts becoming obsessive. |
| 10 | • I’m online and pornography pops up. |
Table 13.2. Fear hierarchy example 2[11]
| SUDs | Triggering Situation |
| 1 | • Questioning my own sexuality at times. |
| 2 | |
| 3 | |
| 4 | • I have noticed that I will check the lock on the door several times most nights even if I have just gone to lock it. |
| 5 | • Difficulty showering/ • Anytime I hear someone take the Lord’s name in vain I mentally say “gosh” because I don’t want to mentally repeat that by hearing it in my head. |
| 6 | |
| 7 | • I like things clean, minimal, put away. I don’t like clutter. Feels overstimulating/ |
| 8 | • Worry about even being alone with someone of opposite gender—fear of flirting/ |
| 9 | • Worry about physical contact with anybody regardless of gender. • Unwanted unclean thoughts about anybody/ |
| 10 | • Worrying about past—guilt, shame—being “clean.” • Being perfectly honest—particularly with my wife—confessing. • Difficulty sleeping next to my son. Scared of being aroused and making myself touch him. • Checking—sometimes I will check myself when I am scared I have become aroused. • Arousal holding, or any physical contact with, my sons (even just holding their hands). • Changing diapers, putting lotion on my sons. Anything like that. • Having my kids sit on my lap. Basically, anything that could cause contact to me, or to them. |
You’ll typically begin your exposures with one of the items on your fear hierarchy somewhere between a four and a six, depending of course on the severity of problem, and your willingness and motivation. As the client, you will always choose and retain agency over the exposure process. Perhaps choose one that is frequently troublesome, so making initial progress will have a noticeable positive impact on your quality of life.
Here are four notes about choosing your initial exposure content as you consider beginning exposures:
1. None of my clients have chosen to spend their time on an exposure when it was only listed as a one or a two on their fear hierarchy. They didn’t feel like that was going to be useful in moving them toward their therapy goals. Those issues didn’t really bother them much, hence the rating of one or two, and they knew how to handle them or work through them. So starting too low on the hierarchy may not feel helpful to you.
2. If you’re not ready to face fears higher up on the hierarchy, I would suggest you need to look at those later. There’s a fine line between a legitimate readiness issue and avoidance. If you’re at the beginning of your therapy process, and you just cannot face a fear that is rated as an eight, nine, or ten on your fear hierarchy, it’s likely a legitimate readiness issue. It would be therapeutically beneficial to start your exposure process at a lower place on the hierarchy so you can more easily have a successful exposure experience, learn to trust the process of exposure, and see that it actually works for you. Then when you move into exposures higher up on the fear hierarchy (those scarier exposures), you’ll have confidence and will likely be more willing to push through the initial discomfort of the increased anxiety as you start the exposure.
3. As mentioned in the previous chapter, please know that you do not need to go through your hierarchy of fears in numerical order.[12] Certainly life doesn’t throw your triggers at you in order! You might start with an exposure that triggers you at a five or six. You will work that same exposure repeatedly over time until it loses fearful power over you. When you see that it is no longer triggering your fear or you start to get bored, you may feel it is time to move on to entirely different exposure content. (Hint: If you are bored, you are not feeling strong anxiety.) Maybe the next time you decide you need to do a new exposure, you drop down and do work with a fear that is a four on your fear hierarchy, and then maybe next time you jump up to a seven. You can change it up and work through things as you deem appropriate.
4. You will likely find that as you work through certain fears, other fears will naturally drop down on the fear hierarchy and not trigger your anxiety as much as they did when you first constructed the chart even though you haven’t explicitly addressed the content with their own exposures. For example, a fear that was ranked a seven on your fear hierarchy initially may slide down to a four through the process of working other exposures, making it much easier to turn your attention to it and take it on in exposure. This is a great sign of progress because it shows you that it is the process of anxiety that is at the heart of therapy, not the focus on the content of the fearful stimulus. Working through the process of exposures naturally tends to reduce fear in many areas.
Overcorrection: a strategy to consider implementing in exposure
Overcorrection is a therapeutic principle that encourages you to tolerate more extreme exposures than are necessary for effective therapeutic progress in typical daily living. To give a weightlifting metaphor, if you get used to lifting twenty-five-pound dumbbells, lifting twenties becomes easy.
For example, one client had difficulty washing his genitals in the shower for fear of the behavior being or becoming masturbatory in nature. He had a history of pornography and masturbation that caused problems in his marriage, including the threat of his wife leaving. Showering caused extreme self-doubt as he obsessively analyzed his intentions for washing his genitals, always wondering if his intentions were sexual in nature. Anything potentially sexual in nature was associated with his core fear of losing his family. Overcorrection in exposure was helpful here as he began showering multiple times per day over some weeks and months. On days when he showered only once, he would wash his genitals twice during the shower. Clearly, showering multiple times per day is beyond what is necessary for him to be able to take care of his typical hygiene needs, but successfully showering multiple times built his confidence against the anxiety. He described his hard-won progress as follows:
Each shower, I grew to loathe the moment that I knew I was supposed to wash myself. I was so scared that many times I just avoided it. I wouldn’t even wash my genitals—and if I did, I would literally do the fastest swipe of the hand and call it good. My anxiety would be so unbearable in that moment that it took everything inside of me to even accomplish that simple task. Truly, my fear and anxiety was completely unbearable. I had to meet that level of fear with the same level of overcorrection. I committed to washing myself multiple times per day. At first it was very difficult. Gradually the fear and anxiety dropped and today, about a year later, sometimes I don’t even think about it when I wash.
As I look back on how distressing showers used to be, I am so grateful I have gotten over this toxic irrational fear. My obsessive and compulsive safety behaviors had trapped me in what felt like an anxiety-constricting straitjacket. I truly was held hostage from doing something as simple as washing myself. Relief, confidence, and peace are the result of consistently overcorrecting in my exposures.
With overcorrection, you provide yourself room for backsliding (such as if you have a busy week or a week of sickness that prevents you from working on therapy) without negative impact on your functioning. In those more extreme exposures, you are also providing a more conservative test where you can experience the likelihood of your feared consequences occurring to be much less than originally feared.[13]
Treatment plan
Once you choose which triggering situation you will begin working with first, take time to write down your treatment plan. Record your distress level (SUDs rating) and the triggering situation from your fear hierarchy. Then label your obsessive fear and the ritual you are targeting in the exposure exercise. Then record what you will do for exposure. Lastly, record how you will prevent yourself from responding. You may want to create some sort of chart, like the blank one in table 13.4.
Table 13.4. Blank exposure treatment plan[14]
| SUDs | Anxiety Trigger | Obsessive Fear | Compulsion | Exposure | Response Prevention |
After you effectively work through your first exposure over some time and you feel ready to tackle another exposure task, you can then select another triggering situation from your fear hierarchy and create a plan for that exposure. Your treatment plan chart may end up looking like table 13.5, which gives you an example of what some of the items from the client fear hierarchy in chart 13.2 could look like in treatment.
Table 13.5. Exposure treatment plan example based on client fear hierarchy (table 13.2)
| SUDs | Anxiety Trigger | Obsessive Fear | Compulsion | Exposure | Response Prevention |
| 4 | I have noticed that I will check the lock on the door several times most nights even if I have just gone to lock it. | “Did I just lock it? Is it fully locked?” | Go back and check the lock; lock and unlock both locks repeatedly | Lock the door once before going to bed | Go upstairs and go to bed; just keep walking; let it go |
| 5 | Difficulty showering/ | “Was my intention sexual?” | Avoid washing or do the quickest swipe with the hand | Wash genitals in the shower. Shower twice per day or wash genitals twice during one shower. | Keep washing. Notice urges to avoid but keep going. |
| 8 | Worry about even being alone with someone of the opposite gender. | “I’m afraid I’m flirting or being disloyal to my wife.” | Avoid being around or alone with other women, even at work. Don’t look women in the eye. Don’t act normal (avoid using any humor). | Interact with other women just like I interact with other men. Talk to them, look them in the eye, use humor. | Do not ruminate over intentions. Keep practicing. |
| 10 | Arousal holding, or having any physical contact with, my sons (even just holding their hands). | “Am I a pedophile?” | Avoid holding my sons on my lap, or if I do hold them put them off to the side mostly on one leg. Or don’t bathe or dry them. | Create multiple opportunities per day to hold boys (holding them at the kitchen table or watching TV), and set them directly in the middle of my lap over my genitals. Change messy diapers. Wash and dry my sons when they need a bath. | Keep holding boys even if I get nervous. Keep working with my wife to bathe and care for our sons. Don’t try to analyze my intentions. |
Rate of exposure
The goal of exposure and response prevention (ERP) is to gradually expose yourself to your obsessions in a safe and controlled manner. Therapy will then become more intensive as you demonstrate an ability to handle your obsessions. Gradual exposure is like dipping your toe into the water at the pool to test how cold it is, and then slowly going in deeper and deeper until you are completely immersed. You start with something on the easier end for one of your more mild or moderate fears and then increase the difficulty of the exposures a bit at a time.
There is another OCD treatment called flooding. Flooding is like jumping straight into the deep end of the swimming pool, choosing to work immediately with the deepest, most difficult fears first, and then working on them until they are overcome. Flooding overwhelms the nervous system to reset it. Flooding and graded ERP seem to be equally effective.[15] Flooding is not part of the current CBT protocols.[16] Some say that ERP is the opposite of flooding.[17] The gradual approach of ERP is the first-line treatment for OCD. It is not quite as intimidating as flooding because it helps OCD sufferers to build up their confidence as they see that ERP works for them. Then they work up their fear hierarchy to the big exposures that address their deepest fears. The examples I’ve provided in this book have followed ERP’s graded exposure.
Length of an exposure session
How long do you need to spend doing an exposure? Initially, you’ll want, if possible, to reach that level of habituation. Stay in the anxiety-provoking situation until your anxiety subsides. Eventually exposure to the obsessional cue will arouse little to no anxiety. It may be the case that you may start to feel more comfortable during an exposure and then your anxiety spikes back up. Just allow the exposure process to be what it is. If your anxiety spikes up again, just keep working through the exposure, trying to allow your thoughts and feelings to be what they are, and allow that anxiety to trickle its way back down again.
Once you begin the exposure process there is a large time demand. You will need to make a commitment to spend the time necessary to complete exposures if you want to reach your therapeutic goals. For the most part, your exposures are going to take a substantial amount of time. In my private practice, initial exposures are often around forty-five minutes or so, although clients may take up to two hours on an initial exposure. Additional exposures may range from fifteen minutes to an hour and a half.[18] Researchers examining exposure in children recommended the maximum exposure length to be thirty to forty-five minutes.[19]
As you work through your exposures, exposure times generally shorten; an initial forty-five-minute exposure can become a fifteen- or twenty-minute exposure after a week or two. Please note that in my experience, a fifteen-minute exposure usually represents the time it takes to allow the anxiety to come down when somebody is nearing the end of a particular exposure process for a feared stimulus. Perhaps the person has been doing exposures for several weeks on this feared thought and the thought is not triggering the anxiety the way it used to. That’s a clue that the person has made great improvement and may be nearing the time to shift to another exposure.
How much time should I spend on exposure practice each day?
Exposure is a demanding part of the therapeutic process. Some people struggle to dedicate sufficient time for their exposures to meet their therapeutic goals. It may be helpful to consider how much time you spend each day ruminating, obsessing, replaying, avoiding, or ritualizing. Is it too unreasonable to dedicate even a portion of that time to your scrupulosity therapy?
One research study assigned clients two hours of in vivo and imaginal exposure each day for the days they did not attend a treatment session.[20] I would agree with that length of time as an ideal. However, most of my clients do not devote that much time to their therapy assignments each day. And, admittedly, most of my clients would also agree that they could probably find more time in their schedules for more exposure practice than they currently do. Remember that your progress in therapy will largely depend on these exposure practices and it comes down to an issue of priorities. Recognize that the more you put into your exposures, the more you’ll get out of them in terms of therapeutic progress. However, if you can dedicate only one hour a day you will still make progress; it will just be slower. One of my clients made great progress in therapy but then began to stall out due to additional time pressures (e.g., applying for new jobs, working on a side business) that kept crowding out his therapy time. He began to backslide on the gains he had made in therapy. Once he began to prioritize his therapy again, doing some type of therapeutic exercise every day, he quickly began to experience lower distress and greater confidence and hope.
Frequency of exposures
You want to schedule your exposures frequently and as close together as possible, practicing exposure two times per day if possible. Those working with children should use shorter but more frequent exposure sessions.[21] If you are not able to do two full-length exposure sessions due to scheduling problems or getting interrupted in some way, I would recommend two or more shorter sessions or one longer exposure in the same day. Sometimes my clients will opt to do a full exposure every other day when they have a busy schedule. Everything you can do is better than what you can’t do, so if that is all you can afford in your schedule, do it. However, your progress will be slowed; the fears will likely diminish more slowly.
Also, it is often the case that if you let your exposure efforts lapse for a few days you may experience a return of fear or an extinction burst (i.e., anxiety that had diminished bursts back up again in a sudden yet temporary manner).[22] An exposure that felt easy the last time you did it may be initially harder to do again (e.g., “Wow! This feels really scary again. Why is my anxiety so high trying do this again?”). This may occur because as time passes, what you learned from the experience of the exposure fades a bit for you—you are less able to access what you learned from the previous exposure to help carry you through to the next exposure. As time progresses without another exposure practice session, what you learned from the previous exposures becomes less and less accessible if you are not continually practicing it.[23] Keep the exposures going and claim your confidence and peace.
Identify the feared consequence
As you begin your exposures, it is important to identify your specific feared consequence. Since anxiety is known for being vague about the dreadfulness of the behavior or thought you fear, it will be up to you to be specific. “If I do [this] . . . I fear [this].” For example, if I hold this knife, I am afraid I will stab myself. Then throughout the exposure process, in addition to tracking your anxiety levels with your SUDs ratings, you can assess whether the feared outcome has occurred: “Have I stabbed myself yet? Am I planning to stab myself?” You can also notice that your capacity to tolerate the distress associated with exposure itself has changed.[24]
A note of caution: Don’t seek to control your anxiety during exposure
Before you begin conducting exposure, I want you to be aware of a difficulty some of my clients have had in enacting exposure. During the initial exposure, and then during the time afterward working through your response prevention (i.e., resisting the compulsions), allow the anxiety symptoms and feelings to be what they are without trying to make them do anything. Thought control, thought neutralization, or thought suppression maintain OCD processes. Do not use exposure as an effort to control your thoughts or to try to force the anxiety to go away. Allow the thoughts to come closer. Accept them as thoughts, acknowledge that they are free to come and go as they will, and that you need not to be threatened by them. Researchers have described the acceptance process as taking what is offered in the moment “completely [and] without defense.”[25]
The reason I make this cautionary note is because I’ve had some clients who tried to use exposure to make the thoughts go away. If you have that ulterior motive, if you are determined to control the thoughts by making them go away, exposure will become a battle and will likely be less effective. It is true that exposure is difficult. Your anxiety will go up initially—and that’s on purpose. As you continue the exposure, your anxiety might come down quickly, or it might not. Just allow it to be whatever it needs to be in that moment. Allow yourself to have an experience with your anxiety. As you stay in the exposure long enough, the anxiety should come down, but you are not to try to force it to come down.
Conducting Exposure
Written exposure
The first exposure I will teach you is called a written exposure,[26] and it’s a very good first step in treating horrific thoughts that feel unbearable. You can use a lined piece of paper and draw a vertical line down the right side of the paper so that you have a very wide column on the left side and a narrow column on the right side of the paper. You are going to write a distressing thought in the wider left column. Then in the narrow column, you’re going to use a number to rate your anxiety level. How much anxiety or distress do you feel as you think about and write down that thought? This is your SUDs (Subjective Units of Distress scale)[27] rating, and it represents the subjective intensity of the distress you are experiencing. You saw on chart 13.2 that researchers used a one to one hundred scale. I tend to prefer a one to ten scale. You can choose your own rating system. You just want to keep track of how your anxiety changes during the exposures so that you have some data to go on and you’re able to remind yourself the distress does go down and it does get better as you go through your exposures.
After you’ve written your initial sentence and rated your SUDs, you’ll move to the next line. In the left column you’re going to write that thought again (ignoring the rating column on the right), and then you’re going to go down to the next line and write your sentence again. Keep up that pattern. After you’ve written the thought a total of ten times, move over to the narrow column and rate your anxiety again with a SUDs rating. You are going to continue this process, page after page, until your anxiety level has diminished by at least half. I generally have clients shoot for an ending SUDs rating of three or four (or thirty or forty) before quitting an exposure. You may spend up to about an hour a day doing this written exercise.
For example, figure 13.6 shows you a page of this type of written exposure. A client in his thirties wrote the fearful thought: “Maybe I will lose my family.”
Figure 13.6. A client’s written exposure exercise[28]
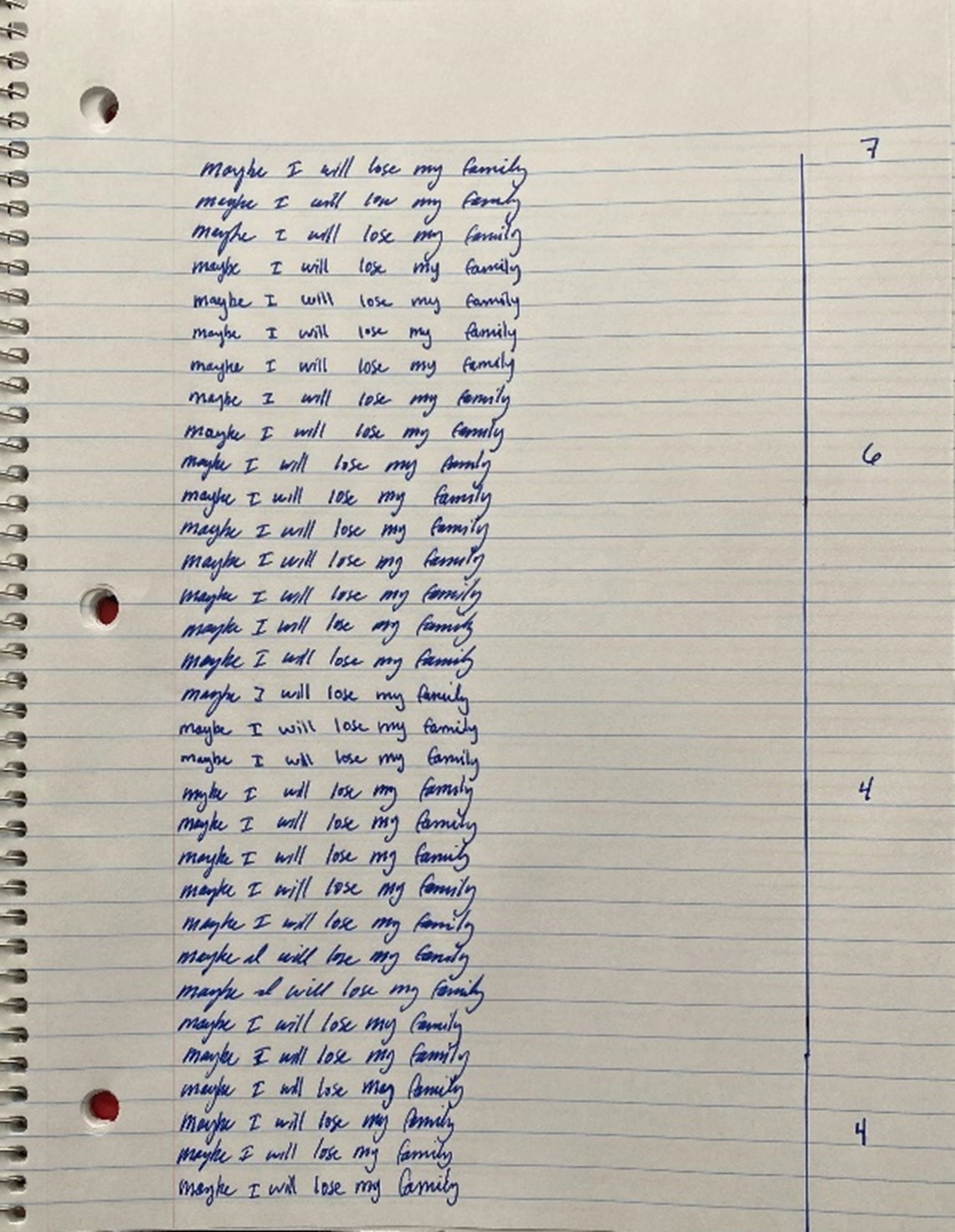
This feared outcome triggered his anxiety when he would obsess over whether content he saw online was pornography or not. As you can see, the first time he wrote this, the triggering sentence created a SUDs of seven. By the end of the page, his SUDs had decreased to four.
You can also modify this exercise to fit your needs. I’ve included figure 13.7, which shows how a female client in her twenties wrote two different sentences that to her were particularly triggering: “What if I choose not to make the same covenants that my family makes?” and “Maybe I’ll leave the church.” She didn’t write in a particular pattern but just freely wrote, writing one sentence until she felt not as engaged and then switching it up to write the other sentence to improve her engagement. She rated her anxiety every five minutes, recording those ratings in a file on her computer.
Figure 13.7. A client’s written exposure exercise modified to fit her needs[29]
Intensive audio exposure
Another exposure exercise you can do is called an intensive audio exposure.[30] You can choose two or three horrific thoughts and make an audio recording of each thought in turn. Take the first thought, saying it slowly about twenty times in a row with a two-second pause after each repetition. Try to add a bit of drama and expressiveness in your voice as you record. If you just talk in a monotone voice or speed through it quickly without emotion in your voice, it probably won’t be as helpful. Continue recording repetitions of that thought until your anxiety has reduced by at least half. Then listen to the thought that you’ve recorded on an endless loop. (There are free apps online that allow you to do this, so you don’t have to keep restarting your recording.) Keep listening to the repeated thought for thirty minutes to an hour per day, or until your anxiety is low. So you’re going to do the full exposure process as written here for one thought. And then when your anxiety is low and you feel it is time to move on, you’ll do this exposure exercise for another thought, and so on.
Total immersion audio exposure
A total immersion audio[31] is like the intensive audio, but it allows you to give more passive attention to the feared stimulus. For this exposure exercise, you’re going to record your horrific thoughts as in the previous exercise, but instead of taking one thought at a time, you’re going to record one thought about twenty different times and then follow that with twenty repetitions of the other thought or two (if you have two or three). Once you’ve made your recording, you’ll listen to that on an endless loop while doing other daily activities for a minimum of about three hours per day, for a week to ten days.
Three hours may sound brutal, or near impossible, but realize this is a more passive approach, so you can utilize your NET (No Extra Time). NET is a concept taught to me by a client. You can do something productive, even therapy assignments, while you are already doing something else that you have to do but doesn’t take all your mental attention. For example, you can put your earbuds in and listen to your exposure content while you’re doing your dishes or your laundry, or going golfing, or walking across campus. You can listen (without earbuds for safety) while driving in your car. Just try to turn on the recording and listen to it anytime you can throughout the day. In this way, you can squeeze quite a bit of therapy time into your day, even though you may genuinely have “no extra time” for therapy.
With this listening exposure, it is not necessary to give the recorded material your undivided attention, but pay attention as often as you can. You may realize at some point you’ve been listening to it for a while and haven’t been paying attention much, so then you may bring your attention back to what you’re listening to in the recording. You may in a few minutes find that your mind has strayed again, but that is okay—just try to listen as best as you can. The key here is really to get a large portion of time during your day where you’re listening to these exposures.
Imaginal exposure—writing your narrative
I’ve referenced imaginal exposures and talked about imaginal exposure narratives. I’m going to walk you through how to construct an imaginal exposure narrative that you can use as a guide for formal imaginal exposure sessions. The template is a more comprehensive, structured way to create an imaginal exposure so you don’t have to wonder what you should include that might be helpful.
You first write down the triggering circumstance (what happened or what is happening). If you think back to our thought chart in our cognitive technique section, this is just like your row A, an objective statement of what happened to trigger your anxiety. Then you write down your initial fear (automatic thought)—that’s your row B on the thought chart. Then you write down your emotional and physical symptoms (consequences). That’s our row C on our thought chart. So those initial sections of the imaginal exposure template should be fairly easy for you to identify and write down.
After that, you write down any additional thoughts that follow from your initial thought that you’ve already recorded (what other fearful thoughts come up for you). Then you write down any compulsive urges you have, without following through with (compulsions or safety-seeking behaviors you want to do but can’t or won’t). And then you write down what it would say about you if your initial fear came true (if the worst happened). The “worst” in this exercise is typically identified by the initial fearful thought you already recorded. Lastly, go a layer below that. Record what it would say about you if your initial fear came true and identify your core fear about the issue. Play out for yourself why it would be so scary, so threatening to you, if this fear came true.
This template can be used for anyone struggling with unbearable, horrific thoughts. What does this look like with a client with scrupulosity? I’ll walk you through an example.
Imaginal Exposure Template
- The triggering circumstance: My girlfriend is going through the temple to receive her endowment next week and I have to go with her.
- Initial fear: I’m absolutely terrified. I don’t feel worthy or ready to go. I don’t feel like I deserve to enter the house of Almighty God. I feel so anxious and petrified. I’m filled with dread, and I am desperately hoping for some way to be okay.
- Emotional and physical symptoms: I’m filled with panic as I think about all the horrible sins I’ve committed.
- Additional thoughts: As I dwell on my first temple experience, I wonder if I was ever worthy to be endowed in the first place.
- Compulsive urges without follow-through: The only possible way I could go would be to meet with my bishop just before and confess all my sins, but that would only worsen my OCD.
- What this would say about me if my initial fear came true: However, if I dared to enter into the temple of Almighty God unworthily, I would be directly mocking God and His power. I would be disgracing my covenants.
- Core fear: I would be drinking damnation. I’m terrified of condemning my soul to an endless misery and suffering. I’m haunted by past guilt and have no idea what God will do to me if I go or went through the temple unworthily. I can’t imagine wasting my eternal potential and being separated from my family and being thrust down to hell all because I didn’t want to love worthily and blatantly disregarded God’s commandments.[33]
Once you’ve written down the responses to each of these stimuli, you then remove the prompts and combine your responses into one cohesive paragraph. Here is the completed imaginal exposure narrative:
My girlfriend is going through the temple to receive her endowment next week, and I have to go with her. I’m absolutely terrified. I don’t feel worthy or ready to go. I don’t feel like I deserve to enter the house of Almighty God. I feel so anxious and petrified. I’m filled with dread, and I am desperately hoping for some way to be okay. I’m filled with panic as I think about all the horrible sins I’ve committed. As I dwell on my first temple experience I wonder if I was ever worthy to be endowed in the first place. The only possible way I could go would be to meet with my bishop just before and confess all my sins, but that would only worsen my OCD. However, if I dared to enter into the temple of Almighty God unworthily, I would be directly mocking God and His power. I would be disgracing my covenants. I would be drinking damnation. I’m terrified of condemning my soul to an endless misery and suffering. I’m haunted by past guilt and have no idea what God will do to me if I go or went through the temple unworthily. I can’t imagine wasting my eternal potential and being separated from my family and being thrust down to hell all because I didn’t want to love worthily and blatantly disregarded God’s commandments.[34]
Researchers have observed that imaginal exposure is helpful when core OCD fears are difficult to address with in vivo exposure. It can be helpful in treating scrupulosity to expose people to these core fears and also assist them to increase their tolerance of acceptable risks. The goal in constructing the imaginal exposure is to create scenarios in which people are engaging in relatively low-risk behaviors that they fear will end up causing catastrophic circumstances.[35] So when writing an imaginal exposure, do not make the scenario unrealistically extreme from the outset. It may interfere with your ability to engage in the scenario and prevent activating your fear so that the exposure doesn’t really prove helpful. Your “scenario should depict realistic behavior that results in an unlikely but feared consequence.”[36]
Here is an example from a client that was a first-year medical student with obsessive-compulsive fears related to reproductive organs (both female and male), as well as some other bodily obsessions. When her anatomy class and dissection lab began covering the internal and external reproductive systems, her anxiety became almost unbearable (about nine on a ten-point scale of discomfort). Lecture slides contained diagrams and photos of the reproductive organs, her professors lectured about them frequently using the reproductive labels, and she and her female lab partner were assigned a male cadaver for dissection. To expose her to the idea that these reproductive words and body parts do not have additional risk attached to them, but are like other body parts, such as elbow, knee, tongue, or digestive tract, she first needed to simply be able to hear and say the words penis and vagina.
One approach to exposure was an in vivo exposure to say the words over and over for several minutes each day. A second exposure approach was an in vivo exposure going through her anatomy class lecture slides with me during our psychotherapy sessions, teaching me about the intricate details of these reproductive systems, such as identifying the intravaginal and supravaginal parts of the cervix. When we began these exposures, she had never said the words before and couldn’t say them without shuddering and shaking her head in disbelief and disgust. We did each of these exposures for some time, but she continued to struggle with them because of deep scrupulous fears. She created the following imaginal exposure narrative as an adjunct to these in vivo exposures, not only to address her OCD fears at a deeper level but to aid her in her professional training—to be a successful doctor she would have to be able to communicate professionally with her patients about their physical symptoms.
A trigger for me is having to listen to, say, write, or study certain words pertaining to reproduction/
reproductive anatomy, like penis and vagina. This feels wrong and very bad. This is going to make me a bad person if I do this, or even being willing to means I must be a bad person. Saying these words enough might make me like them, and then I would be really bad, or maybe I would realize I liked them all along and then I would have been bad all along and just pretending not to be. If other people heard me [saying these words over and over for exposure] they would think I was really creepy or crazy. I’m afraid I’m never going to be able to get these words to go away and they will trigger other disturbing thoughts. I feel guilty, afraid, and stressed. I feel like my muscles are tense, and I can’t sit still and I feel hot. I want to avoid all these words, but I won’t so I can learn and be a good doctor and help people. If the worst happened, it would say I am a horrible, gross, creepy, perverted person. I am an evil person. I will never be able to get these words/ thoughts out of my head, and then I will get more and worse ones, and then I will act on them and I will probably go to hell.[37]
After continuing therapy for about a year, she had made so much progress—even while remaining in medical school and being forced through her studies to face some of her deepest fears: “I’m lucky in some way that I have access to really interesting big exposures. . . . I had to study for gynecological and male and female genitourinary exams. I am proud of myself. I was going through the flash cards with these words and pictures on them, and I could read them through and have all the words going through my head and it’s almost not a big deal.”
I would encourage you to use the imaginal exposure template in this chapter and work on creating your own imaginal exposure narrative before moving on.
Imaginal exposure—conducting an exposure session
To use the extended narrative for exposure, find a private place and read the paragraph you have written out loud. When you get to the end of the last sentence, pause and evaluate how the narrative struck you. Was it horribly triggering or only somewhat distressing? Rate your distress rating (SUDs) in any place where you choose to keep your therapy data. Once you’ve given it a rating, go back to the beginning and read the narrative again, and then read it again and again and again. Pause and take note of your SUDs level every five or ten minutes, just so you can see how the anxiety may shift throughout the exposure session. Once you rate your SUDs, just go back to the beginning of the paragraph and keep reading until five or ten minutes has passed; then stop to rate your SUDs again. Keep going with this exposure process until you feel fairly comfortable (usually cutting your initial SUDs rating in half) or even until you’ve gotten a bit bored.
For some variation, you can also record this exposure paragraph and listen to the recording in a looped format. You can actively participate with the exposure loop, listening and reading along with your eyes on what you’ve written. Or you can do the more passive approach I’ve already described in which you record it and just listen to it passively for about three hours per day.
Maximize variability to enhance learning
To enhance your exposure outcomes, you can use varying exposures, content, contexts, anxiety levels, and exposure schedules in your exposure exercises. This variability increases long-term retention of safety learning.
You can increase learning in exposure by combining different types of exposure.[38] For example, in self-harm OCD you can use in vivo exposure to expose yourself to knives or scissors. You can also use an imaginal exposure template to work through your worst fears. To increase the strength of safety learning from the exposure, you can combine them and expose yourself to knives or scissors (holding them or having them on the table in front of you) while reading your exposure narrative. With scrupulosity, you can look at a religious image or statue or a photo of one of your church’s leaders while going through an imaginal exposure. “When a feared outcome fails to occur despite the presence of multiple fear cues, it creates strong learned safety to inhibit existing obsessional fear.”[39] This process is called “deepened extinction.”[40]
You can vary the content of your exposure by expressing uncertainty about whether your feared outcome will occur in one exposure practice session, while in another you can express that your feared outcome has occurred. You can also vary the context of your exposure by practicing exposure in as many different situations as possible. You can end your exposures at varying anxiety levels. Instead of doing each exposure until you reach the level of habituation, you can utilize varying stopping points. This will provoke uncertainty when an exposure is stopped sooner than the level of habituation, allowing you to learn that you can tolerate your anxiety at any point, not only when it declines.[41]
Practicing exposure this way can help you consolidate your treatment gains against a potential future relapse. Instead of relying on the belief that “‘I’ll be okay because I know my fear will go away by the end,’” conducting randomly ordered and varied exposures would foster a belief that “‘I’ll be okay because I can tolerate anxiety and uncertainty.’”[42]
Concluding Exposure Sessions
Following each exposure trial, it would be useful for you to take a moment to identify what you have learned from that specific exposure session. What was your experience? You may learn something different each time. Here are some examples from one client, a single woman in her early twenties who recorded what she learned after many of her exposure sessions. Notice the variety of things she learned.
- Uncertainty makes me uncomfortable.
- Funny the fear is so irrational, yet my mind can rationalize it.
- It’s crazy how one word or phrase can induce so much anxiety.
- I should keep recognizing the things that trigger me and then expose myself to them.
- I am powerful. (Thinking about doing exposures every day and how hard it used to be, and now it’s not like a big deal.)
- Feeling anxiety about my exposures is a good and productive thing.
- Apparently this is still a tough thing for me.
- If I am doing exposure I am making progress.
- Doing therapy homework is powerful.
- It blows my mind how I went from sobbing about this to being able to finish in ten minutes without a single tear.
- Consistent exposures work wonders.
- The cool thing about exposures is that you can do them anywhere. Healing is always available.[43]
Here are some examples from another client, a married man in his early thirties who recorded what he learned after many of his exposure sessions.
- These are just irrational thoughts.
- They are just words; they can’t hurt me unless I act on them.
- These thoughts are the opposite of who I am. I don’t need to worry about them or give them energy.
- I need to be able to tolerate living with uncertainty.
- I have an anxiety disorder.
- If I try to make myself or pressure myself to feel less distress and get a lower number as I progress through the exposure, my distress will actually go up.
- I’m making progress. Keep going!
- I’m glad I’m working on my mental health and anxiety disorder. I don’t want to end up divorced, miserable, and alone like my mom. She’s destroyed her relationships with her kids and is all alone because she is so unhealthy. I’m glad I’m doing this and taking care of myself.
- I am really over magnifying the importance of this event. It’s really a nonissue.
- Today I learned that I need to be consistent with doing these every day.
- It’s not distressing—these are irrational thoughts. It’s just words in the background.[44]
You can summarize what you learned during your exposure and also take note of anything that surprised you. Highlighting the discrepancy between what you expected would occur and what actually occurred will be helpful to your therapeutic progress. Specifically, you can examine how your anxiety levels changed throughout the session, how your expected fears may or may not have occurred, and how your ability to tolerate the distress of the exposure may or may not have changed.[45]
Integrating Interventions
The last few chapters have covered quite a few different therapeutic interventions. How might it look to put them together as a self-help treatment approach? Ideally, in any intervention episode you would begin with self-soothing skills, meditation, or mindfulness. This can include healthy coping statements and self-talk. This foundational work will help prepare you for your intervention.
Then you select which therapeutic intervention seems the most appropriate for the situation you are in and the level of anxiety you are experiencing. You may do a thought chart or other types of cognitive interventions, such as challenging distortions in your journal. Or you may select some type of exposure. I typically encourage going from the least invasive intervention that will meet your treatment needs to the most invasive intervention.
When you’re done with your intervention, ideally you would take a moment or two to do some soothing again. If you’ve done your intervention appropriately, your level of anxiety shouldn’t be particularly high if you’ve reached the level of habituation, but the soothing will signal “Okay, now, I’m going to be shifting gears. I’m going to transition to something else.”
After you do some soothing for a moment or two, I would recommend one of your positive-sentiment activities, if even just for even a moment. Remember to maximize your NET (No Extra Time), such as listening to music while you drive. The positive-sentiment activities can be very helpful in changing mental gears from the content of the obsessional fears you were focusing on during the exposure. Exposures can be draining and exhausting. You can bring in a little bit of positivity, and you’ll be able to continue with your daily activities without the exposure bleeding in and taking over the rest of your day (hopefully).
One client put together a list to remind himself of all the things he had learned in therapy so he could more easily act in a therapeutic manner rather than giving in to his fears. He asked the question, “How do I let go of the need for certainty and deep-seated fears (I’m afraid there’s something in my past I need to confess to the bishop; I’m afraid there’s something I’ve done or thought recently that needs to be confessed to a bishop, and all the other ones we’ve talked about)?” He then answered his question with this list. You will see that it incorporates all the treatment elements I’ve discussed in this book.
- Act like I’m worthy
- Pursue my values (not just religious ones)
- Don’t argue with anxiety
- Don’t overanalyze the situation, thought, etc. Try to let it pass (meditation skills)
- Pray for help to let it go
- Do something on my positive-sentiment list
- Do a thought chart
- Relaxation techniques (self-soothing)
- TIP skills
- Do formal exposures
- Do background exposures (total immersion)
- Read through my therapy notes
- Wait it out
- Repeat mantras:
- Faith is not a 100 percent guarantee
- The Savior knows my heart and desires
- The Savior can take care of it
- The Savior knows I would confess if I knew I needed to
- The Savior knows I struggle with anxiety
- The Savior knows I just want to be good and worthy
- Obsessive thoughts in OCD do not equal wish fulfillment.[46]
ERP as a General Lifestyle Approach
Once you have successfully done some exposures, begin to make exposure and response prevention a general lifestyle approach. In addition to working at formal exposure practice, create a vision of the importance of seizing everyday life opportunities to have an experience with your anxiety. I am speaking of leaning into anxiety, rather than leaning away from it whenever the opportunity presents itself. One researcher taught: “Confront, rather than avoid, feared situations that arise unintentionally through the course of the day. In other words, do what OCD tells you not to do.”[47] He calls this “lifestyle exposure” because you are choosing exposure over avoidance as a way of life.
Another researcher commented that you should continue lifestyle exposure to challenge your obsessions even after you have made therapeutic progress and they are just “background noise.” She then shared that one of her clients tossed his bread on his kitchen floor every morning before toasting it for breakfast, just to keep pushing back on his contamination symptoms.[48]
Notes
[1] Abramowitz, J. S. (2001). Treatment of scrupulous obsessions and compulsions using exposure and response prevention: A case report. Cognitive and Behavioral Practice, 8(1), 84. https://
[2] Huppert, J. D., & Siev, J. (2010). Treating scrupulosity in religious individuals using cognitive-behavioral therapy. Cognitive and Behavioral Practice, 17, 386.
[3] Greenberg, D. (1984). Are religious compulsions religious or compulsive: A phenomenological study. American Journal of Psychotherapy, 38(4), 530. https://
[4] Hyman, B. M., & Pedrick, C. (2010). The OCD workbook: Your guide to breaking free from obsessive-compulsive disorder (3rd ed.). New Harbinger Publications, Inc., 182.
[5] Abramowitz, 2001. Treatment of scrupulous obsessions and compulsions, 81; emphasis added.
[6] Huppert & Siev, 2010. Treating scrupulosity in religious individuals, 386.
[7] Greenberg, D., & Huppert, J. D. (2010). Scrupulosity: A unique subtype of obsessive-compulsive disorder. Current Psychiatry Reports, 12, 287–288.
[8] Greenberg & Huppert, 2010. Scrupulosity, 287–288.
[9] Hyman & Pedrick, 2010. The OCD workbook, 79–87.
[10] Client work, used with permission.
[11] Client work, used with permission.
[12] Jacoby, R. J., Abramowitz, J. S., Blakey, S. M., & Reuman, L. (2019). Is the hierarchy necessary? Gradual versus variable exposure intensity in the treatment of unacceptable obsessional thoughts. Journal of behavior therapy and experimental psychiatry, 64, 54–63. https://
[13] Huppert & Siev, 2010. Treating scrupulosity in religious individuals, 386.
[14] Shapiro, L. J. (2015). Understanding OCD: Skills to control the conscience and outsmart obsessive compulsive disorder. Praeger, 113–115.
[15] Boersma, K., Hengst, S. D., Dekker, J., & Emmelkamp, P. M. (1976). Exposure and response prevention in the natural environment: A comparison with obsessive-compulsive patients. Behaviour Research and Therapy, 14(1), 19–24. https://
[16] Keeley, M. L., Storch, E. A., Merlo, L. J., & Geffken, G. R. (2008). Clinical predictors of response to cognitive-behavioral therapy for obsessive-compulsive disorder. Clinical Psychology Review, 28(1), 119. https://
[17] McClean Harvard Medical School Affiliate. (2021, September 24). Everything you need to know about exposure and response prevention therapy. McClean Hospital. https://
[18] Hyman & Pedrick, 2010. The OCD workbook.
[19] Harris, C. V., & Wiebe, D. J. (1992). An analysis of response prevention and flooding procedures in the treatment of adolescent obsessive compulsive disorder. Journal of Behavior Therapy and Experimental Psychiatry, 23(2), 107–115. https://
[20] Abramowitz, 2001. Treatment of scrupulous obsessions and compulsions, 79–85.
[21] Harris & Wiebe, 1992. An analysis of response prevention and flooding procedures, 107–115.
[22] Extinction (psychology). (n.d.). In Wikipedia. https://
[23] Jacoby, R. J., & Abramowitz, J. S. (2016). Inhibitory learning approaches to exposure therapy: A critical review and translation to obsessive-compulsive disorder. Clinical Psychology Review, 49, 31. https://
[24] Jacoby & Abramowitz, 2016. Inhibitory learning approaches to exposure therapy, 32.
[25] Hayes, S. C. (2005). Get out of your mind & into your life: The new acceptance & commitment therapy. New Harbinger Publications, Inc.,45.
[26] Hyman & Pedrick, 2010. The OCD workbook, 171.
[27] Wolpe, J. (1969). The practice of behavior therapy. Pergamon Press.
[28] Client work, used with permission.
[29] Client work, used with permission.
[30] Hyman & Pedrick, 2010. The OCD workbook, 172.
[31] Hyman & Pedrick, 2010. The OCD workbook, 173.
[32] Hyman & Pedrick, 2010. The OCD workbook, 196.
[33] Hyman & Pedrick, 2010. The OCD workbook, 196.
[34] Client work, used with permission.
[35] Huppert & Siev, 2010. Treating scrupulosity in religious individuals, 387.
[36] Huppert & Siev, 2010. Treating scrupulosity in religious individuals, 387.
[37] Client story and work, used with permission.
[38] Craske, M. G., Treanor, M., Conway, C. C., et al. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. https://
[39] Abramowitz, J. S. (2018). The inhibitory learning approach to exposure and response prevention. International OCD Foundation. https://
[40] Rescorla, R. A. (2006). Deepened extinction from compound stimulus presentation. Journal of Experimental Psychology: Animal Behavior Processes, 32(2), 135–144. https://
[41] Abramowitz, J. S., & Arch, J. J. (2014). Strategies for improving long-term outcomes in cognitive behavioral therapy for obsessive-compulsive disorder: Insights from learning theory. Cognitive and Behavioral Practice, 21(1), 28. https://
[42] Abramowitz & Arch, 2014. Strategies for improving long-term outcomes in cognitive behavioral therapy, 28.
[43] Client work, used with permission.
[44] Client work, used with permission.
[45] Jacoby & Abramowitz, 2016. Inhibitory learning approaches to exposure therapy, 32.
[46] Client work, used with permission.
[47] Abramowitz, J. S. (2018). Getting over OCD: A 10-step workbook for taking back your life (2nd ed.). Guilford Press, 139.
[48] Shapiro, 2015. Understanding OCD, 145.
