Self-Help Treatment
Exposure
Debra Theobald McClendon, "Self-Help Treatment: Exposure," in Freedom From Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Provo, UT: Religious Studies Center, Brigham Young University; Salt Lake City: Deseret Book), 221–48.
I introduced the vicious cycle of anxiety in chapter 6. This cycle shows that anxiety provokes you to try to escape or avoid the anxiety-causing trigger using safety behaviors, such as compulsions. That avoidance may feel immediately relieving, but the relief is only temporary and makes things worse in the long term—it reinforces your anxiety, making it harder to resist the urges to ritualize in the future.
Exposure Model Basics
According to the exposure model, to reduce fear you need to activate your fear network. You create systematic, predictable confrontation of a feared stimulus with the aim of reducing a fearful reaction. You face the thing you fear, and then you realize that your feared consequence doesn’t happen or isn’t likely to happen. As you confront the fear, it is defeated. In psychotherapy treatment for OCD, we take basic exposure and combine it with response prevention. This is called exposure and response prevention, or ERP. The foundation of ERP was laid in the early 1900s when famous scientists studying behaviorism, such as Ivan Pavlov and John Watson, used components of ERP while exploring classical conditioning. In 1958 another famous behaviorist, Joseph Wolpe, developed a form of systematic desensitization based on relaxation training. The goal of systematic desensitization was to use exposure to diminish sensitivity to situations that caused fear or dread. It forms the foundation of modern ERP, which was created by Stanley Robinson in the 1970s. ERP was specifically designed to help people struggling with obsessions and compulsions. Over the recent decades, ERP therapy has been refined into its modern form.[1]
ERP corrects overestimates of threat and danger that underlie obsessional-compulsive anxiety[2] by experimentally testing the accuracy of anxious predictions. Here are four beliefs you may have that you can learn are not true through ERP: (1) You may believe that disastrous consequences will occur upon exposure to your fears if you don’t perform your rituals. With ERP you find out that that’s not true. Instead of ritualizing, you can do nothing, and then you learn that nothing bad happens or is likely to happen. (2) You may believe intrusive thoughts are intolerable and must be avoided. With ERP you find out that you don’t have to avoid the intrusive thoughts and you can learn to tolerate them—and as you do, you find the frequency of the thoughts decreases. (3) You may have the belief that anxiety is unbearable and will last forever. But with ERP you learn by experience that anxiety does increase as you go into a feared situation, but if you continue in the anxiety-triggering situation or thought without avoidance or safety behaviors, the anxiety actually goes down on its own without your having to do anything at all. So you find that you can bear anxiety and that it is temporary. (4) You may believe that uncertainty is intolerable. As you test that belief for accuracy through ERP, you find out that although the uncertainty might be uncomfortable and trigger your anxiety (particularly at the beginning of therapy), uncertainty can be tolerated and it doesn’t have catastrophic consequences.
As such, you can see that the ERP process will also help you increase cognitive flexibility. ERP “overlaps with acceptance based therapies that aim to increase one’s willingness to experience unwanted private experiences such as obsessions, anxiety, and fear.”[3]
Reversing the Vicious Cycle of Anxiety: Exposure Is Key
What do you do to reverse that vicious cycle of anxiety? Reversing this toxic self-perpetuating cycle is paradoxical. Instead of following common sense, which would induce you to avoid the thing distressing you to stay “safe,” you must confront it explicitly. Then you prevent yourself from responding with the safety behaviors that you’ve become accustomed to doing to neutralize or suppress your anxiety. You resist the compulsions, mental or physical, that have become your maladaptive responses. Think back again to the painful “battery incident” I shared at the end of chapter 1 and that we discussed again while talking about thought charts in chapter 11. My client’s efforts to get rid of batteries led to digging through a COVID-era public trash can with her child standing guard. It appeared to be a story about the disposal of batteries, but it was really a story about the process of toxic anxiety. This client reflected:
Looking back, I know where I went wrong in the therapeutic process. It wasn’t when I went back to look in the trash or when I researched online for obscure battery laws—although those were problematic in their own right. It was at the very beginning. At the precise moment I looked at those batteries and with anxiety, felt like I had to get rid of them—and get rid of them as quickly as possible. I should have hit the pause button right there. I should have put the cup of batteries in my kitchen to look at for a week (instead of out sight in the laundry room), or I should have driven around with them in my car for days, as therapeutic exposures. I desperately wish I could have seen that from the very beginning. Hindsight is 20/
20, though. I see this battery incident as a learning experience and one step closer in my recovery process.
St. Ignatius began to conquer his OCD by taking an agere contra (doing the opposite) approach.[4] And you will need to do the same. You will do this through exposure, a counterintuitive process of leaning into the fear rather than avoiding it.
Figure 12.1. Reversing the vicious cycle of anxiety[5]

First, as seen in figure 12.1, instead of giving in to the urge to escape your triggering situation, you will confront the fear, but not with the use of any safety behaviors (such as saying a prayer, or shaking your head, or putting your hands in your lap to avoid accidentally touching someone). You will most likely experience a short-term increase in anxiety. This does not mean you are doing it wrong or what you are doing is wrong; it means facing the fear is inciting the anxiety. Then something tends to start to shift. The focus that you have on yourself because of your anxiety symptoms decreases and you can calm down a little bit. The attention scanning common in anxiety, such as scanning for possible threats, also decreases. Then you use your coping skills, which continue to bring the anxiety down to a manageable level. As you see your efforts benefitting you, you then start to feel more confident: “I did this, I can handle this.” And so the next time you have a feared situation, you know from experience that you can tolerate it and use your coping skills and other therapy tools to work through it successfully. One client wrote, “When I do my therapy consistently, I feel confident within myself. I feel like I’m making progress and doing the right thing.”
As you practice having an experience with your anxiety by doing exposure exercises, it is true that your anxiety will initially go up. Understandably, this is the last thing those of you with scrupulosity want to sign up for! One of my clients described it as “putting your hand on the stove and leaving it there until you don’t feel it anymore.” No joke, exposure therapy is the hardest thing I have ever asked clients to do. And yet the discomfort of exposure therapy is short term, while the torture of religious terror and subsequent avoidance compulsions becomes lifelong! This is where you need to keep in mind your long-term goal, trusting that the temporary increase in distress is necessary for you to ultimately have a more lasting decrease in anxiety. You do not have to want to do exposure, you just have to be willing to do exposure.
Figure 12.2. Pattern of anxiety during exposure[6]
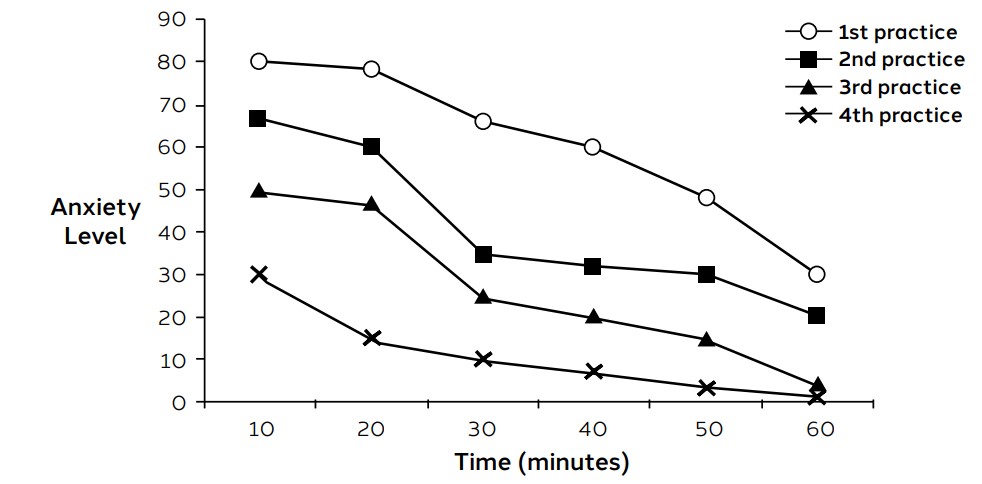
Figure 12.2 shows distress levels of an individual struggling with OCD (this is not scrupulosity specific) during exposure. As you can see, the first anxiety level on the first exposure is just miserable. If you can get yourself through that first exposure, it just gets better from there; the anxiety starting points get lower and lower with each subsequent exposure. The anxiety-level outcome also decreases over the course of the exposure process. You can see that in this example the third and fourth exposures ended with the person reporting almost no anxiety.
Figure 12.3. Subjective anxiety reported during imaginal exposure at sessions 2 and 8.[7]

Figure 12.3 depicts anxiety levels of two exposure sessions for one researcher’s client that was struggling with scrupulosity. The dark line represents the ratings for session number 2 in the treatment process. At the beginning of the exposure session the person’s anxiety was triggered at about a 50 on a 100-point scale. After about five minutes, the anxiety spiked and was significantly higher at a 90 and then was basically at 100 for about fifteen minutes. This is the part of exposure that is pretty miserable. And yet you see that after twenty to thirty minutes the anxiety steadily decreased. After about forty-five minutes, this person rated the distress as a 30, which is in a fairly comfortable level.
The lighter exposure line in figure 12.3 represents session 8 for this same person. The researchers had continued to do exposure at each subsequent session, so the person was getting used to how the exposure process worked and could trust that the anxiety comes down on its own without having to do anything. Here you can see that the initial exposure triggered the person’s anxiety at only a 10 because he or she had done this several times before and was beginning to habituate, or get used to the process. Then as the person got five minutes into the exposure, the content triggered them emotionally and the anxiety spiked up to a 70. But then within only another five minutes after that, the anxiety dropped all the way down to 40, which again is pretty tolerable. After forty-five minutes, the person’s anxiety was barely detectable.
Habituation
While putting ERP into practice, there’s an important principle mentioned above called habituation. When you engage in exposure and your anxiety is triggered and then increases, in time it will begin to diminish. You can become comfortable again or even bored, though you’re still in the anxiety-provoking situation. You have reached the level of habituation, which is a “natural tendency of the nervous system to numb out to stimuli through repeated, prolonged contact.”[8] One researcher commented, “When you expose yourself to the thing you fear for long enough, your anxiety will usually burn itself out.”[9]
“Habituation models posit that fear reduction during an exposure trial is a necessary precursor to subsequent, longer lasting cognitive changes in the perceived harm associated with the phobic stimulus.”[10] For example, if you begin an exposure and your anxiety spikes really high so you cut and run, quitting the exposure, all you’ve done is reinforce the avoidance of your obsessive-compulsive cycle without gaining any of the necessary learning experiences that will prove therapeutic.
One person shared his experience reaching the level of habituation for the first time during an imaginal exposure:
Step by excruciating step, [my therapist led] me through the worst of my fears surrounding the whole . . . issue. For a full forty minutes I imagine out loud every hypothetical disaster that Doubt [the name he used to identify his OCD] can come up with. . . .
And then something happens. I suddenly get very tired of hearing myself talk. I become almost bored with the entire process. Somehow it’s as if I’ve managed to wring out every last drop of anxiety from each of the once highly charged words I’ve been using to describe my very worst nightmares. “Fire,” “flames,” “suffocation,” and so many others of Doubt’s vocabulary favorites could now just as easily be flavors of ice cream; they have lost all their emotional meaning to me.[11]
Habituation is a noticeable milestone for clients. In my experience, once clients have had this experience, they seem to “trust” the therapy process more implicitly.
As you do exposures repeatedly, they will help promote healing in time, but one exposure session will not be a magic wand curing all your anxious complaints. In fact, the first exposure will probably be the most miserable since you are not accustomed to the process and don’t trust it yet. You can encourage yourself with coping statements such as, “It’s good practice to let go of this worry. I want to practice.”[12] It should get better and better each time—anxiety generally won’t trigger as high and tends to resolve more quickly (exposures get shorter). Eventually the exposure to the obsessional cue will arouse little, if any, anxiety.
My clients tend to be very nervous about doing exposure “right.” They want to know for sure how to discern when to end their exposures, so as not to limit some of its utility by ending the exposure prematurely. I teach them to stay in the exposure long enough to have their anxiety come down to where they feel generally comfortable. But since that guideline is not concrete enough for some, I then suggest staying in the exposure a few more minutes until they get bored. And then, with a smile on my face, I push the scenario to a bit of ridiculousness, indicating that they should then continue the exposure another few minutes until they feel irritated at me for telling them to do it so long! That seems to get a smile and resolves the concern.
Inhibitory Learning Model of Extinction (or Inhibitory Learning Theory)
Although there is wisdom in spending a good amount of time in your exposures, additional research suggests that reaching the level of habituation is not always necessary for effective exposure practice.[13] Another emerging field, inhibitory learning theory, proposes that therapeutic exposure operates on an extinction model rather than a habituation model. Habituation leads to a reduction in fear following repeated presentations of an anxiety trigger during treatment. This is a form of non-associative learning, whereas extinction is a form of associative learning. During an exposure, a person confronts an anxiety trigger and the feared prediction does not occur. This changes the person’s expectancies about the likelihood that such fears will occur and leads to behavior change, such as a reduction of fear.[14] One researcher offers this explanation:
ERP teaches new information about safety so that following successful exposure, a feared stimulus has both its original fear-based meaning (“door knobs are dangerous”) as well as the new safety meaning (“door knobs are generally safe”). In order to be optimally effective, ERP needs to help people learn safety in such a way that it is strong enough to block out (or inhibit) the original fear—and this is where the term inhibitory learning gets its name. Fear extinction is maximized when a person uses ERP to learn new safety information that inhibits existing obsessional fear. The goal of ERP is therefore to learn safety in a way that permanently inhibits obsessional fear.[15]
This model has found that timing of the exposures and other factors may be more important than the level of fear one is experiencing at the end of an exposure (the focus of the habituation model). It may be the case that shorter, more frequent exposures are more important than whether you reach habituation in any given exposure.[16]
Inhibitory learning is accomplished by implementing eight strategies:[17]
- Challenge your expectation of what you think is going to happen during the exposure and pay attention to what actually happens. What did you learn?
- Eliminate safety behaviors.
- Practice exposure in multiple contexts.
- Label your emotions during the exposure (rather than going on what you assume you will feel).
- Switch up the order of exposures on your fear hierarchy. Life doesn’t throw anxiety triggers at you in order.
- Work toward deepened extinction by doing exposure in multiple locations or scenarios in which your anxiety could resurface.
- Reconsolidate, meaning go back and remember your fears while you are bringing in new data with the exposure. New learning occurs and memories can be altered.
- Reinforce the extinction when the feared consequence may actually happen by staying within your window of tolerance. Take it in stride.
Conditions for Effective Exposure
Some people may erroneously believe that if they have experienced accidental exposure or occasional chance exposure to their feared stimuli and are still afraid, it means exposure therapy will not work for them, but this is not the same as exposure. One OCD researcher outlines four conditions to consider:[18] (1) Exposure needs to be intentional; it won’t work if it’s accidental. (2) Exposure needs to be prolonged; if it’s too quick you won’t be able to have an experience with your anxiety and learn what you need to learn. (3) Exposure is not a magic wand, solving your problems after one exposure effort. The exposure needs to be repeated. As you test your expectations over and over and over again, you need to see that your feared outcome is not likely to occur. (4) If an exposure does not trigger your anxiety, it will not be helpful. It must cause some anxiety and uncertainty. Notice the feelings, but remember not to fight them or try to make them go away.
As you can see, exposure takes purposeful attention, time, and energy. It is a demanding treatment. As you consider these conditions for effective exposure, also check yourself on your commitment and follow through to act in a values-centered manner. One person reflected on the real reason he didn’t make progress in therapy for a protracted length of time:
When I look back on my own circuitous path to recovery—what I did right, what I did wrong—it’s obvious now where I fell short for so many years: I did everything necessary to get better except the hard work. . . . Yes, I showed up at my therapist’s office week after week, but I did the bare minimum necessary to convince her I was on board with her program; and . . . I lied to her about the homework I was doing in between visits. And then I got frustrated because I wasn’t getting better!
If there’s one thing I’ve learned from my recovery experience, it’s that when it comes to escaping Doubt, there are no shortcuts.[19]
Types of Exposure
There are several types of exposure that you may utilize in your journey toward robust mental health. I will discuss interoceptive (symptom) exposure, in vivo (situational) exposure, imaginal exposure, and virtual reality exposure.
Interoceptive exposure
The word interoceptive means “relating to stimuli produced within an organism, especially in the gut and other internal organs.”[20] Interoceptive exposure means to expose yourself to the physical, internal symptoms that are common to your anxiety. For example, if your heart begins to race when you have anxiety, you may become sensitive to that sensation so that any time your heart begins to race you begin to panic. So you can create an exposure that simply causes your heart to race. You can walk or run up and down the stairs, you can watch an exciting or scary movie, you can engage in sexual activity, or other heart-racing experiences. Experiencing the increase in heart rate and realizing that your feared expectations do not come true or are not likely to come true, noticing that just having your heart beat faster it is not threatening, can be an effective exposure. Then in future moments when you find yourself in an anxiety producing situation and your heart begins to race, you won’t be as fearful of the sensation, which may help you avoid panic.
Other types of symptoms you can treat with interoceptive exposure include flushing or nausea. If you get facial flushing when you’re anxious, you can get in a hot tub, sauna, or hot shower. If you feel sick to your stomach—nauseated—when you’re anxious, you can watch others donate blood or donate blood yourself, watch a surgery video, or even watch videos of people eating gross foods (you can find all sorts of hideous things online!).
You can also use interoceptive or symptom exposure for symptoms that are not explicitly tied to your anxiety but are connected to your anxiety through your fear. I am specifically talking about the physical sensation of sexual arousal. Many of my clients are afraid of their own sexual arousal—particularly the fear that if they notice a sensation of sexual arousal in any circumstance, then they are guilty of sin. For example, maybe you’re doing some exercises and notice a slight sensation of arousal and then panic about what it means. Instead of being afraid, you can choose to take it on therapeutically through interoceptive exposure. One client was concerned about this issue while working out. We had him work out more! These were very effective exposures, and he gained a great confidence over his anxiety. After pushing through the initial blip of sensation, he didn’t notice anything again because he was working too hard! It teaches the lesson “Okay, that’s fine. It’s no big deal. I can move on.”
In vivo (situational) exposure
In vivo (New Latin for “within the living”), or situational, exposure involves creating a direct confrontation and experience with the feared stimulus or anxiety trigger. If you fear elevators, you will ride elevators. If you fear large crowds of people, you will go the theater, large lecture halls, or to large sporting events. If you fear germs, you will touch items your OCD has declared “dirty” (exposure) and then not wash your hands (response prevention) for some length of time.
Twelve points[21] summarize the recent research on maximizing your efforts to produce therapeutic in vivo exposures. They include some principles already presented of the inhibitory learning model:
- Practice exposures that match the anxious trigger in reality as closely as possible. Failing to do so can sabotage the exposure.
- Use your exposure practice to test your predictions. Think about what you are afraid will happen in the exposure, and then conduct the exposure as an experiment to find out if your fears are correct.
- Continue with the exposure until you’ve learned that your fears are unlikely to be realized and that you can tolerate anxiety and uncertainty about the fears (not necessarily just to a level of habituation where you feel more comfortable).
- You should expect to feel discomfort, such as anxiety or uncertainty during your exposure practice.
- Use your exposure time to embrace your anxious feelings. You are creating an experience with your anxiety. By confronting it, it diminishes.
- Don’t try to control the obsessions. OCD treatment is paradoxical; the more you accept the presence of obsessions, the less power they start to hold in your life.
- During exposure, don’t ritualize or try to neutralize your anxiety, but do use response prevention. If you ritualize during or after exposure, you are unable to test the accuracy of your fearful predictions. It will render exposure less helpful.
- Don’t use distraction or self-soothing during an exposure. Since the point of the exposure is to have an experience with your anxiety, if you’re not paying attention, you won’t learn anything. Stay fully engaged in the present moment.
- During exposure, rather than seeking out data to reassure yourself that everything will be okay, take risks and get surprised by what you learn.
- Practice exposure daily since the more you put into your exposure work, the more you’ll get out of it.
- Create variety in your exposure practice. Rather than working through your fears in order of severity, feel free to mix it up.
- Practice your exposures in different settings so you can apply what you have learned through exposure to a variety of situations as they arise throughout your day. If you limit your exposure to one setting, it may have limited transferability.[22]
How can we apply in vivo exposures to work with scrupulosity? Prior to meeting with me, many of my clients have chosen to severely restrict the media they consume, so much so that they can permit themselves to only watch church content or listen to religious music. For an in vivo exposure, you can watch television or movies that your scrupulosity has deemed off limits or listen to popular music. Just reading movie reviews can be an effective exposure. Just because it triggers your anxiety does not mean it is inappropriate (remember that emotional reasoning is a distortion). The media may be benign, but if it is triggering anxiety in a very significant way for you, then this type of exposure should be quite useful.
If you’re having scrupulous fears about chastity, immoral thoughts, or pornography, you can practice “good touch” with family or loved ones, such as brushing hair, holding hands, hugging, cuddling, or sitting next to them on the couch while your thigh touches their thigh. Or you may shop for bathing suits online or watch beach/
Early in my therapy, we planned an exposure to help me overcome my fear of sexual or inappropriate thoughts by shopping for modest women’s swimsuits. I would basically go to a website and look through pages and pages of modest swimsuits with models until I felt my initial anxiety decrease. This was a valuable exposure because I felt there was some risk involved. That risk was very difficult and uncomfortable, but I noticed that as I stuck with it, my anxiety eventually went down.
One thought I like to focus on with risky or uncomfortable exposures is to remind myself that my Heavenly Father wants me to make improvements to my mental health, and that He perfectly understands my situation. I had to trust that my therapist wouldn’t ask me to do anything against my moral standards, and that God knew the process of anxiety and what I needed to do to weaken its influence on my life.
If your scrupulosity has declared certain topics off-limits, you can choose to have an uncomfortable conversation with someone on a topic that your scrupulosity has deemed unacceptable. The possibilities are endless here—honesty, politics, abortion, LGBTQ issues, self-harm or suicide, thoughts about a Sunday School lesson or church sermon, and the like.
To address scrupulous fears with an in vivo exposure you can also choose to read bothersome material. This may be addressed two ways: First, sometimes reading doctrinal material from your own church canon or church leaders can trigger anxiety and panic over a myriad of issues. If this is the case you can continue to read the material, such as the scriptures, over and over again until you become more comfortable with it. I have also had clients watch a small video clip of a doctrinal message that triggered them and then loop that piece of the video to watch it over and over and over again. A client recalled an experience along this line:
The first big exposure I did during treatment was to watch a video of an apostle speaking on the importance of keeping myself worthy and clean. It’s a beautiful video, but it speaks and shows very candidly the importance of being worthy, or becoming worthy if you aren’t already.
I watched and listened to that video over and over and over again. It was an interesting journey, because my anxiety did not always behave linearly. Some days I would watch and feel more anxious than others. There were times that I felt that I could watch the video and not feel anxious at all, just to find myself struggling with the video the next day.
After some time, I remember one day at work I had time to listen to a talk. I decided to do an exposure with this video. As I listened to it, I felt that the talk was unobscured by anxiety and I actually felt the Spirit. I felt happy listening to the very thing that had thrown me into an anxious mess so many times before. I even felt prompted about someone I felt I could reach out to and help.
Second, sometimes your scrupulosity has deemed certain nonreligious material or all nonreligious material on the fringe or even unacceptable. If you lean into the anxiety and read the material in a purposeful therapeutic exposure practice, you can come to realize that the material was not the problem—it was your anxiety.
You may also make a therapeutic goal to remove reliance of repeated intrusive repentance prayers. For this example, I want to show you how this could look in an unethical exposure and then how the exposure could be modified to meet your treatment goals while also ethically considering your religious beliefs.
For a prescribed time, you could stop praying to break the compulsivity of the prayers. The halt on prayers would only be temporary while you were working on the issue in treatment. This type of intervention would be effective to break the obsessive-compulsive cycle, but it would also create a lot of dissonance for those who care very deeply about their relationship with God. In addition, the doctrine of many religious traditions commands their believers to pray.[23] So designing an intervention to omit a religious requirement is not ethical. In this situation the exposure would likely become a double assault on you emotionally: (1) the loss of the compulsive repentance prayers would increase your anxiety, as exposure is meant to do; but (2) not praying would also provoke legitimate guilt (in contrast to toxic guilt) because you’ve elected not to follow one of the commands of your religious dogma. For most, the increase in anxiety is plenty difficult to manage, without needing to cause additional distress.
One way I have modified this exposure to help clients break the compulsivity of their prayers is to change the nature of their prayers. Many scrupulous individuals are trapped in a process of just “begging” God for forgiveness all the time. The prayers are completely self-focused on their own spiritual terror. If you find that this is also your case, you can continue your prayers as you typically do them, but then put restrictions on the content of your prayer—that it cannot include anything about repentance or forgiveness or helping you to do better at some perceived failing. “Prayers said as meaningful expressions of faith and religious identity (even those that bring about solace in a general sense) are not part of OCD and do not need to be stopped during treatment.”[24] If you can’t keep compulsively repenting, what can you pray for? Express gratitude to God for the many blessings in your life; take time to identify some of those blessings. Have you ever tried a prayer in which you only expressed gratitude? You can also pray for your family members (by name) or pray for other people. Pray over your church assignments and stewardships. Pray to be successful in your work, school, home duties, and commitments. Pray to ask God to help you to prioritize your scrupulosity therapy or to have the courage to do your exposures.
The idea with this exposure is not that that you won’t ever repent again in your prayers (which would also violate religious requirements and provoke guilt rather than anxiety), but that while you are in the throes of scrupulosity and anxiety is corrupting your spiritual experience, you have a hard time discerning what is a genuine sin that requires repentance and what is anxiety or scrupulosity. So you halt the repentance first for a specified time.
You can liken the process to pushing a pause button. If your resist the urge to confess or repent compulsively, and the issue was solely triggered by anxiety, in a couple of days the issue will likely be completely gone. Many of my clients have found after pushing the pause button that when they went back to acknowledge the issue they were anxious about a few days earlier, they couldn’t even remember what had distressed them so terribly. Contrarily, if the issue is a legitimate sin for which you should repent, then after you’ve paused and come back to it the Holy Spirit will still be there to prompt you: “You know, this is really something you should look at.” The Spirit is the spirit of truth, and it will give you the emotional space to ponder and work through this. Then when you’re through the exposure you can go back and say something like: “Okay, Heavenly Father, I realize I did this thing. I’m not sure it was the best thing to have done. I haven’t talked to you about it yet and repented because I was in the middle of my treatment, and I wanted to make sure I was seeing it as clearly as possible, that it was a legitimate issue. But now I do want to acknowledge this. I want to express that I’m sorry for this and I will work to do better.” Don’t worry, you won’t have missed your only chance to repent. If it’s truly a legitimate issue needing your spiritual attention, it’ll still be there. The exposure is not a denial of repentance, but it’s simply a pause until you can see things more clearly.
I had one client who expressed positive feelings about the exposure of halting compulsive repentance prayers. He said, “It was nice. Prayers haven’t been as repetitive. Instead of always just begging for forgiveness all the time, prayers are more meaningful.” You are also doing this exposure for the sake of connecting more genuinely with God. Jesus teaches in the Bible to avoid the use of “vain repetitions.” “But when ye pray, use not vain repetitions, as the heathen do: for they think that they shall be heard for their much speaking.”[25] “The New American Standard Bible translates ‘vain’ as ‘meaningless.’ Compulsive prayers are rote incantations of words, done for no other reason than to put right an obsession. They do not reach out to God. They are, as the Bible tells us, self-centered and hollow. As a general rule, OCD sufferers should strive never to repeat a private prayer more than once.”[26]
Another way to modify the prayer exposure would be to put time limits on your prayers to break the compulsive confessing and repenting that just goes on and on and on. Perhaps you feel unwilling or unable to stop all repentance in your prayers at this time, but you can see and agree that the inordinate amount of time you spend praying for forgiveness and spiritually battling with God is unreasonable. You may decide to allow yourself some compulsive repentance praying for the first few exposure sessions until you feel confident enough to eliminate it.[27] Perhaps you are spending hours and hours every day in prayer. You can limit yourself to thirty minutes or an hour total per day in prayer. You would use a timer or stopwatch to monitor your time in prayer. Once you’ve hit the maximum time allotted for prayers, you are done praying for the day and will have to wait until tomorrow to pray again. So even if you haven’t restricted the confessing completely, you are working toward breaking the compulsive cycle that is thieving so much of your life from you.
As you get used to the initial time restriction on your compulsive prayers and it gets easier for you to keep your prayers within that new allotted time, you can then shorten the time limit again, to maybe fifteen or thirty minutes total prayer time per day. Once you have successfully reduced your compulsive praying down to a length of time that is a reasonable, it may be much easier to then omit all unnecessary repentance content.
One client who was constrained by feeling her prayers had to always follow a prescribed pattern reported the following after some weeks of in vivo exposure aimed at helping her change her prayers: “Practicing therapy exposures has been anxiety inducing as it has encouraged me to face my fears around praying in the wrong order, but I have felt more free and even relieved when I don’t have to say this prayer ritual the same way every time.”
Imaginal exposure
Imaginal exposure is an exposure technique in which you directly confront your core fear(s) or worst-case feared stimulus with imagery[28]—mental images, thoughts, memories, words, ideas, and the like. For example, one client who was fearful that he would feel unworthy when he was married in a temple used imagery to imagine being in a temple getting married. He pictured what the room would look like, he pictured family and friends who would be there, and he pictured the wedding ceremony. This exposure was done even though he was single. Once he became engaged and was preparing for marriage, he was then also able to be more specific in his imagery by picturing his bride there with him. He commented: “I really appreciated the opportunity to be proactive with imaginal exposures. Practicing these imaginal exposures helped prepare me to get engaged, attend the temple, and feel confident about being sealed in the temple. I wouldn’t have been able to reach these important milestones without intentionally exposing myself to those ideas when I was single.”
Imaginal exposure is particularly helpful when it might be unethical, impractical, or difficult to conduct a direct in vivo exposure. Imaginal exposure is very helpful in the treatment of scrupulosity because oftentimes we can’t do a direct exposure. How do you do a direct in vivo exposure addressing fears such as “I’m afraid I’m a totally damaged person,” “I’m afraid I’m going to lose my family forever,” “I’m afraid I’ve disappointed God,” or “I fear eternal damnation”? The imaginal exposure also helps the client learn to tolerate acceptable risks.[29] Lastly, the imaginal exposure helps you tap into core fears that may not necessarily be activated during an in vivo exposure. For these reasons, we heavily rely on imaginal exposure in scrupulosity treatment.
Virtual reality
Virtual reality exposure combines elements of in vivo and imaginal exposure to create a virtual, or computer-generated, simulation of a feared situation or object. The feared stimulus looks real but is not.
Virtual reality exposure can prepare you for later exposures in real-world settings, but it can also be a sole method of exposure delivery. For example, you could use virtual reality exposure to treat a flying phobia when the time and financial cost of purchasing and taking frequent flights is prohibitive. Virtual reality exposure has the advantage that you have greater control over the exposure process; you can repeat exposures as many times as is necessary (which is not always possible in a real-world setting), you can control variables so additional anxiety triggers do not arise, and you can personalize the exposure environment.[30]
Virtual reality has been shown in review studies to have similar drop-out rates and similar outcomes as in vivo exposure, except for one review that showed in vivo exposure to have better outcomes.[31] These studies were done with social anxiety disorder and not OCD, so we should be cautious about drawing any conclusions. Furthermore, to the date of this printing, there have been no studies of virtual reality for the treatment of scrupulosity. Virtual reality could be helpful in scrupulosity treatment to address a fear for which an in vivo exposure would also be helpful; however, it would likely have limited utility for fears that require imaginal exposure
Taking an Appropriate Level of Risk
If you struggle with germ and contamination OCD, your anxiety wants a guarantee that if you touch something you’re not going to get sick. It tells you, “If you touch this, the consequences are catastrophic.” OCD brain malfunctioning causes a sense of dread with its faulty alarm system misfiring, so you feel like you’ll end up in the emergency room of the local hospital or end up dead after a simple touch . . . of anything. The anxiety is loud and scary in its demands and threats, but it’s also vague. It doesn’t actually tell you the specific details of what will happen to you if you touch “it.” You likely can’t articulate what you are really afraid of, but it’s just how you feel. It feels like it is going to be bad! And the cognitive distortion of emotional reasoning tells you that since you feel that way it will be bad.
There is always a kernel of truth in obsessions—no matter how unlikely it is that the feared outcome may occur, there is still the possibility that it could. Since OCD wants a guarantee that you’re not going to get sick, it tells you not to touch anything. So you obey and you don’t touch anything. Maybe you don’t get sick physically (maybe you still do), but at what cost? Your life gets boxed up as tiny as can be and you are trapped inside the box—you’ve lost a robust and healthy life and instead become paralyzed. A teaching by Saint Julie Billiart (1751–1816) pushes back on this idea. She taught, “Better mistakes than paralysis.”[32]
OCD grossly exaggerates the actual stakes at risk. OCD lies. With germ and contamination OCD, even if you were to get sick from an exposure in which you touched something your OCD labeled as “dirty” or “contaminated,” the chances of going to the emergency room or dying from the exposure are pretty much slim to none. It is true you might get sick, but if so, you’d probably only get a cold, which is entirely manageable. So we take an appropriate level of risk to work on pushing back the OCD, noting that it is possible you could get sick after the exposure, but the risk is pretty small—it’s just not probable. Instead, you can recognize that the minuscule risk is worth the large gain of reclaiming your mental health.
One researcher and clinician made an astute observation regarding the quirkiness of toxic anxiety: When a feared outcome does actually occur, the person, ironically, does not panic and assault himself or herself with blame. Instead the person responds rationally and focuses on what needs to be done to address the problem.[33] I have observed this dynamic in my clients as well. A difficult occurrence pulls them out of their future-oriented “what-if” mentality and requires them to fully engage in the present moment. The panic of so many unknown yet anticipated moments is replaced by the calm of one known moment—even though that moment was previously the focus of so much fear and anxiety.
What is an appropriate level of risk in scrupulosity?
In scrupulosity, toxic anxiety tells you that if there is any detail missed in a confession, or any inadvertent sin committed for which you may not have repented, the consequences are eternally catastrophic, such as eternal damnation or loss of exaltation. Scrupulosity OCD wants a guarantee that you will be saved. It encourages frequent confession and constant replay. That type of fear is not amenable to expectancy testing in the way that germ and contamination OCD is, and so you end up in the same place again and again struggling with this uncertainty. “If only I could remember every sin . . .” So if you could remember every sin and confess them all, is that a guarantee of salvation? What if you sin again tomorrow? And the day after that? What if . . . ? What if . . . ? Researchers have indicated that scrupulosity tends to be more difficult to treat because therapists may try to use treatment to disprove feared outcomes, when the scrupulous feared outcomes are impossible to prove or disprove (e.g., “Am I a pedophile?”). In addition, some of the obsessions involve expectations that are long-term (e.g., “If I don’t remember every sin, I will be damned eternally”). Instead, these researchers recommend that
exposures for these presentations of OCD should be reframed to identify (and violate) more immediate expectations, which are often overlooked. These include the expectation that one will not be able to tolerate (a) thinking obsessional thoughts, (b) uncertainty about the feared consequences, and/
or (c) anxious arousal associated with confronting feared stimuli. Specifically, expectancy tracking can be used to help patients exceed their expectations about being able to continue exposure while feeling anxious, uncertain, and having obsessions.[34]
Following this counsel to make exposures more relevant to current expectations, still offers no guarantees. You might fearfully ask, “What if I do this exposure and I might be sinning?” As you accept the possibility of sin, anxiety tends to, paradoxically, go down. To accept the uncertainty of sin, you need to take an appropriate level of risk. In OCD exposure treatment, you don’t just go out and blatantly sin on purpose and call it exposure—that’s not going to be helpful for scrupulosity. Sin triggers guilt, not anxiety. Therefore, we don’t expose you to sin. We exposure you to the fear of sin.
In scrupulosity, uncertainty is heightened because in most scrupulous issues you cannot reality test your expectations. Even if you have done any number of things that could threaten your spiritual standing before God, religious doctrine accounts for it, such as with the principles of atonement or forgiveness. But OCD struggles to tolerate the uncertainty of faith. Instead, scrupulosity will likely threaten you that you are going to be unworthy, and the feeling of dread experienced with that accusation is that because of that unworthiness you will lose everything. Scrupulosity will falsely skew your understanding of religious doctrine and say that you better not leave your salvation in the hands of a “poorly understood” faith process—that it is too risky. It will lie to you and tell you that you better take more control and be more hypervigilant so you can save yourself. Remember that toxic anxiety lies. Trust the therapeutic process and take the risks necessary to move toward healing. “The treatment itself is scary because it requires you to take risks that are so averse to you that you have organized your life around avoiding them. However, these risks are acceptable, and no greater than risks that healthy, happy, successful people take many times on a daily basis.”[35] If you are feeling hesitant to take risks, a coping statement may be helpful. [36] For example: “If those without OCD can take this risk, then I can too.” Or, “My compulsions don’t really keep me safe the way I think they do. I can change the way I deal with my fears.”
Notes
[1] McClean Harvard Medical School Affiliate. Everything you need to know about exposure and response prevention therapy. https://
[2] Foa, E. B., & Kozak, M. J. (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99(1), 20–35. https://
[3] Buchholz, J. L., Abramowitz, J. S., Blakey, S. M., et al. (2019). Sudden gains: How important are they during exposure and response prevention for obsessive-compulsive disorder? Behavior Therapy, 50(3), 674.
[4] O’Flaherty, V. M. (1973). Therapy for scrupulosity. In R. M. Jurievich (Ed.), Direct psychotherapy: Twenty-eight American originals (pp. 221–243). Miami University Press, 234.
[5] Government of Western Australia Department of Health. (n.d.). Anxiety—reversing the vicious cycle. https://
[6] Abramowitz, J. S. (2018). Getting over OCD: A 10-step workbook for taking back your life (2nd ed.). Guilford Press, 90. Used with permission. [TS: Use the hi-res version provided.]
[7] Abramowitz, J. S. (2001). Treatment of scrupulous obsessions and compulsions using exposure and response prevention: A case report. Cognitive and Behavioral Practice, 8(1), 82. https://
[8] Hyman, B. M., & Pedrick, C. (2010). The OCD workbook: Your guide to breaking free from obsessive compulsive disorder (3rd ed.). New Harbinger Publications, Inc., 56.
[9] Burns, D. D. (2006). When panic attacks: The new drug-free anxiety therapy that can change your life. Morgan Road Books, 259.
[10] Craske, M. G., Treanor, M., Conway, C. C., et al. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 11. https://
[11] Bell, J. (2007). Rewind, replay, repeat: A memoir of obsessive-compulsive disorder. Hazelden, 265–266.
[12] Foa, E. B., & Wilson, R. (2001). Stop obsessing! How to overcome your obsessions and compulsions. Bantam, 88–89.
[13] Abramowitz, J. S. (2018). The inhibitory learning approach to exposure and response prevention. International OCD Foundation. https://
[14] Jacoby, R. J., & Abramowitz, J. S. (2016). Inhibitory learning approaches to exposure therapy: A critical review and translation to obsessive-compulsive disorder. Clinical Psychology Review, 49, 28–40. https://
[15] Abramowitz, 2018. The inhibitory learning approach to exposure and response prevention.
[16] Craske, M. G., Treanor, M., Conway, C. C., et al. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. https://
[17] Shapiro, L. J. (2020). Obsessive compulsive disorder: Elements, history, treatments, and research. Praeger, 104–105.
[18] Abramowitz, 2018. Getting over OCD, 171–172.
[19] Bell, J. (2009). When in doubt, make belief: An OCD-inspired approach to living with uncertainty. New World Library, 104.
[20] Google Dictionary, s.v. “interoceptive.” https://
[21] Abramowitz, 2018. Getting over OCD, 173–177.
[22] Abramowitz, J. S., & Arch, J. J. (2014). Strategies for improving long-term outcomes in cognitive behavioral therapy for obsessive-compulsive disorder: Insights from learning theory. Cognitive and Behavioral Practice, 21(1), 20–31. https://
[23] See Ephesians 6:18.
[24] Abramowitz, J. S., & Hellberg, S. N. (2020). Scrupulosity. In Storch, E. A., McKay, D., & Abramowitz, J. S. (Eds.), Advanced casebook of obsessive-compulsive and related disorders: Conceptualizations and treatment (pp. 71–87). Academic Press/
[25] Matthew 6:7.
[26] Osborn, I. (2008). Can Christianity cure obsessive-compulsive disorder: A psychiatrist explores the role of faith in treatment. Brazos Press, 164.
[27] Levy, H. C., & Radomsky, A. S. (2014). Safety behaviour enhances the acceptability of exposure. Cognitive Behaviour Therapy, 43(1), 83–92. https://
[28] Berman, N. C., Summers, B. J., Weingarden, H., & Wilhelm, S. (2019). Positive affect and imaginal exposure processes in patients with taboo obsessions. Journal of Obsessive-Compulsive and Related Disorders, 23. https://
[29] Huppert, J. D., & Siev, J. (2010). Treating scrupulosity in religious individuals using cognitive-behavioral therapy. Cognitive and Behavioral Practice,17(4), 387.
[30] Kent, C. (2021, August 3). Virtual reality meets OCD with tech-enhanced exposure therapy. Medical Device Network. https://
[31] Anderson, P. L., & Molloy, A. (2020). Maximizing the impact of virtual reality exposure therapy for anxiety disorders. Current Opinion in Psychology, 36, 153–157. https://
[32] Beattie, T. (2011). Scruples and Sainthood: Accepting and overcoming scruples with the help of the saints. Loreto Publications, 39.
[33] Shapiro, L. J. (2015). Understanding OCD: Skills to control the conscience and outsmart obsessive compulsive disorder. Praeger, 81.
[34] Jacoby & Abramowitz, 2016. Inhibitory learning approaches to exposure therapy, 33.
[35] Purdon, C., & Clark, D. A. (2005). Overcoming obsessive thoughts: How to gain control of your OCD. New Harbinger Publications, 65; emphasis added.
[36] Shapiro, 2015. Understanding OCD, 151.
