Self-Help Treatment
Cognitive Work
Debra Theobald McClendon, "Self-Help Treatment: Cognitive Work," in Freedom From Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Provo, UT: Religious Studies Center, Brigham Young University; Salt Lake City: Deseret Book), 195–220.
In this chapter, I share specific cognitive interventions you can do to promote peace, healing, and wholeness. Exercise your faith by pursuing evidence-based therapeutic interventions to treat your scrupulosity OCD.
Cognitive Model
Let’s look at scrupulosity from the cognitive model—the perspective that anxiety comes from distorted, illogical thoughts or self-talk. According to the cognitive model, if you’re having anxious thoughts then you feel anxious, you’re telling yourself some things that are not true (distortions), and you’re buying it. When anxiety is out of control, thoughts are particularly fraught with a myriad of these types of distortions. These distortions restrict cognitive flexibility. Yet you can learn different ways to respond. “Erroneous beliefs and interpretations are only one of several possible ways of reacting to obsessional triggers and thoughts.”[1] So, from the cognitive model, if you change the way you think, you change the way you feel.[2]
Cognitive Distortions
Cognitive distortions are tendencies in our beliefs or thinking patterns that are false (or are not fully accurate) and cause emotional distress and harm. Many of these distorted, erroneous thoughts happen so quickly they feel automatic. Cognitive distortions[3] are thinking patterns that all people tend to find themselves in occasionally; these are not limited to those with OCD. Even if you do not yourself struggle with scrupulosity, perhaps you will see here some “pet” distortions of you own. There are many types of cognitive distortions; however, here I will share a few that are prominent in scrupulosity.
- Emotional reasoning. You reason from the perspective of how you feel—your feelings are facts. Examples include: “I feel unworthy, so I am unworthy.” “I feel guilty, so I am guilty.” “I feel anxious, so something is wrong.” With emotional reasoning, you are not in your Reasonable Mind, but in your Emotional Mind.[4]
- Personalization (self-blame). You blame yourself for things you’re not entirely responsible for. One of the reasons I see clients personalizing and blaming themselves is because acknowledging that something is really somebody else’s issue, or that somebody else has the ability to control a situation, makes the client feel powerless. But the client who takes the blame tends to believe, “If it was my fault, then maybe I can fix it.”
- All-or-nothing thinking. This is black-and-white thinking, in which things are seen in absolutes. For example, “If I’m not perfect, then I am the worst.” This is a particularly prominent cognitive distortion in OCD and explains much of the intolerance for uncertainty (the gray area).
- Labeling. This is generalizing the totality of your identity from a single data point, such as one mistake or flaw, with one broad stroke (e.g., “I’m evil”). Labeling is a problem because it doesn’t allow you to be anything else, whereas if you evaluate your behavior and can say, “I made a mistake—here’s how I could have done this better,” then you’re able to work on improvement for the future.
- Jumping to conclusions. You come to a conclusion that is not based in fact. There are two types of this distortion:
- Mind reading. You assume people are reacting negatively to you even though you don’t have any evidence.
- Fortune-telling. You arbitrarily predict that things will turn out badly. Anxiety is biased, keeping you scanning for threat. Threat assessment is high, so everything feels threatening, and that goes into your predictions.
- “Should” statements. You criticize yourself or others with “shoulds,” “musts,” “oughts,” and such (e.g., “I shouldn’t have done that” or “I should have known better”).
- Magnification or minimization. You blow things way out of proportion; on the converse, you shrink their importance.
Other cognitive distortions may include concepts such as double standards. Additionally, remember that the three cognitive domains found specifically in OCD (as discussed in chapter 5) are also distortions: responsibility and threat estimation, perfectionism and intolerance for uncertainty, and importance and control of thoughts.[5]
These distortion patterns are emotional amplifiers, meaning they gain intensity through repetitive thought. If we have an anxious or fearful thought, and we engage in distorted thinking around that thought, it will simply amplify that fearful emotion, making it stronger and stronger and stronger until we’re completely flooded and overwhelmed and our emotional stability deteriorates.
Therapeutic Cognitive Exercises
Here I introduce you to six cognitive exercises you can do to address your anxiety: conducting a cost-benefit analysis, challenging distortions, examining definitions, creating a thought chart and a responsibility pie chart, and transferring responsibility to God. There are many types of cognitive interventions available. If these exercises feel useful to you, I encourage you to seek out additional resources.
Cost-benefit analysis[6]
A cost-benefit analysis can help you pinpoint stuck points (think: distortions) and provide motivation. You list the advantages and disadvantages of a particular thought, feeling, or habit. Then you compare the two lists, balancing them against each other.
For example, you can think of the advantages that will come if you move forward with scrupulosity treatment. Most of the time when you think about your OCD, you probably think about your pain and the reasons you feel it is necessary to obey OCD’s demands. Here you can explore all the disadvantages—all that the OCD has cost you. How have you been hurt by your OCD? You can examine things like lost or wasted time, opportunities you may have missed, embarrassing situations you’ve found yourself in, events you’ve been late to, financial or employment losses, damaged or lost relationships, pathological guilt, and other hardships.[7] You can then also think of the disadvantages of engaging in scrupulosity therapy. You may discover hidden benefits your OCD provides you that are holding you back from entering in or fully engaging in OCD treatment. Your lists may look something like the list in table 11.1.
Table 11.1. Cost-benefit analysis for doing OCD treatment
Advantages of Treatment | Disadvantages of Treatment |
|
|
80 | 20 |
Once you’ve made the two lists, you can then rate the relative weight or value of the content of each list, making the two lists add up to one hundred points. Perhaps the list of possible therapy advantages is very heavily significant to you, so you rate it an 80, while the list of disadvantages may have several items on it that are not as important to you, so you rate that list a 20. (Rather than rate the entire list, it may be easier to consider and rate each item individually.) This can help clarify some of the unspoken issues that may be driving you.
Challenging distortions
Another cognitive method is to challenge distortions through Socratic questioning. I’ll use examples of three cognitive distortions to show the types of questions you can ask. First, there are a lot of double standards held by those suffering with scrupulosity. They may understand the doctrines of their belief, and they can see how these doctrines apply to other people, but they cannot see how those doctrines could possibly apply to them. One client sadly said, “Jesus is the Savior, but not mine.” The overemphasis on the doctrine of justice to the exclusion of any mercy or grace is a poignant example here. So this is a double standard. You can challenge the distortion: “Is it fair to have harsher rules for yourself that are different from your rules for everyone else?” Or “What would you say to a friend who had a harder set of rules for herself than for other people?” Or “What does holding double standards do to your self-esteem and mood?”[8] Or “Would you ever tell your friend that he is beyond the love and grace of Jesus?” Second, Socratic questioning for the cognitive distortion of overgeneralizing can look like this: “How does it follow that someone’s worth as a person can be judged on one instance of not meeting a goal or making a mistake?” Or “What do most people judge as important in making up a person’s worth?”[9] Third, another distortion that you can challenge is the “should” mentality. You can ask, “How does saying ‘should’ to yourself constantly make you feel? In what way does it impact your sense of self?” Or “What impact do you think it might have if you apply the sort of pressure you apply on yourself to a close friend?”[10]
Examine definitions
In addition to challenging the distortions through Socratic questioning, you can examine the definitions of the words you are using. Does the word you are using really mean what you are taking it to mean? What does it mean to be “evil,” a “fraud,” “immoral,” a “gross” person, or a “bad mother”? One researcher counseled:
Ask yourself what those labels mean. If you try to define what you mean . . . you’ll usually discover that one of four things is true:
- The label applies to all human beings.
- The label applies to no human beings.
- The label is inherently meaningless.
- The label doesn’t apply to you.[11]
As you think about applying this approach specifically to your scrupulous concerns, you may want to examine definitions of various other words or phrases such as: good enough, sinful, unlovable, unredeemable, unworthy, wicked, and so on. For example, one client expressed an insight that came to him about the word worthy: “Worthy is not a feeling.”
Thought charts
You can also challenge distortion through the use of a thought chart. A thought chart is a cognitive tool allowing for a structured, organized approach to thoughts that can so frequently be fast and chaotic in OCD. This tool helps you identify the presence of any distortion in your thinking and then dispute the distortion with contrary evidence. This leads to more reality-based feelings that can be acted on more appropriately. For example, in scrupulosity, you can separate OCD behaviors from behaviors that are more appropriate expressions of true religious or spiritual belief.
Figure 11.2. Thought chart
A | Activating Event | ................................................................................................................................................ |
B | Belief | |
C | Consequences | |
D | Dispute | |
E | Eliminate | |
F | New Feeling | |
G | Go and Do! |
Thought charts are common therapeutic tools. If you search online, you can find many different examples. Here is one type of thought chart that I’ve put together. (I have included a larger version of this in appendix 4 that you can copy and use for your own cognitive work.) Working through an example will make this easier for you. Figure 11.3 shows you how one client, a single man in his early twenties who had been in therapy for about six months, filled out a thought chart about a sexual thought triggering scrupulous anxiety for him.
[CC: In the chart below, make straight quotes and apostrophes curly. In row D, line 5, change comma after “sinful” to semicolon. In line 6 add comma after “thought.” In row E change “%” to “percent.”]
Figure 11.3. Client thought chart 1[12]
A | Activating Event |
|
B | Belief |
|
C | Consequences |
|
D | Dispute |
|
E | Eliminate |
|
F | New Feeling |
|
G | Go and Do! |
|
Row A is the activating event. This is simply a place to record the objective event that occurred, triggering your anxiety. For this individual, the anxiety trigger was “a sexual thought popping up.” Row B is your personal belief about that event. Or you can identify your automatic thoughts about the event. As you can see, this man had three different automatic thoughts or beliefs about this activating event, as he recorded them in row B: “This is sinful.” “I shouldn’t be thinking that. If it comes up, I must want it.” “This is pornography.” You can see that the thoughts are all related, so we left them all together to address in the same chart. (If you have several thoughts, but they are completely different from each other, I suggest splitting the thoughts into two completely different thought charts.) Row C represents the consequences of the automatic thought. The consequences can be both emotional consequences (e.g., I cried, I felt guilty, I was angry), or they can be behavioral consequences (e.g., I left the room, I hit the wall, I cried, I isolated myself, I did compulsions). For this client, the emotional consequences were “feel[ing] guilty, anxiety, fear of offending God.” The behavioral consequences were “avoidance compulsions, praying, distraction.” These three rows, A, B and C, are simply a description of your lived experience. A: Something happened. B: You had thoughts and beliefs about that something. C: Consequences unfolded from your reaction to that something.
With this chart, you’re going to work to break that cycle of reaction and create a healthier pattern by learning how to respond rather than react. The most important row in the thought chart is row D. This is where the therapeutic change begins to happen as you work to infuse flexibility into your thinking. You’ve likely spent much of your life looking for evidence to support the assumption that you have in row B (confirmation bias). Here you will learn to do the opposite; you are going to find evidence to disprove your assumption. You will dispute the assumption you have in row B and say why it is not 100 percent true. This may be difficult at first because you are working to do the opposite of what you have done for so long. But with practice your cognitive flexibility will improve, and the process will become easier.
If you look back to the client’s chart in figure 11.3, you see that in row D he worked through a variety of detailed evidence from a variety of angles that disputed his distorted beliefs in row B. His disputes were as follows: “As humans we are sexual beings as well as divine sons and daughters of God.” “I can’t control every thought that comes into my head, but I can decide what I do with it.” “Men tend to be sexually-oriented for connection and affection.” “Looking for pornography is actively seeking it for sexual pleasure. I am not doing that.” “I am at sexual prime. Having the thought or instinct is not sinful; it’s how I’m wired.” “Even if I did want to think this thought, it doesn’t merit confession to a bishop.” “I am biologically programmed to be this way.” “Emotional reasoning (‘I feel unworthy, therefore I am’) is a distortion.” “Temptation is not a sin.”
Please try to work through disputes without letting obsessive-compulsive energy take over. One of my clients learned this the hard way when she turned a thought chart into a two-and-a-half-hour exercise. She never wanted to do a thought chart again! Once I limited her to thirty minutes of work on a thought chart, this intervention became helpful to her. You don’t have to be exhaustive with your disputes. You just need evidence from a variety of angles to begin the work of unseating the distortion in your row B thought and hopefully getting some emotional buy-in.
Now let’s move on to row E. In row E, you’re going to eliminate the distortion present in your previous row B thought by creating a new, more reality-based thought that summarizes the essence of what you learned from your disputes in row D. You’ll create one idea that you can use to replace the distorted thought in row B. My clients generally take one of two approaches: (1) read through all the disputes and create a sentence summary, or (2) take one dispute that is particularly powerful and just copy and paste it over. As you see in the client example, he summarized what he learned in row D with two related thoughts: “I can’t control 100 percent of the thoughts that come in.” “Just because a thought comes in doesn’t mean I am guilty.”
After processing through rows D and E, how are you feeling? Has anything shifted for you? In row F you will list any new feelings, a contrast to the emotional and behavioral consequences you previously listed in row C. If you indicated in row C that you were feeling guilty, anxious, or depressed, perhaps after doing the work of row D and row E you are now feeling more peaceful, steady, or confident. Maybe the shift isn’t quite so dramatic, but you are less anxious. Maybe you don’t really buy it yet (the disputes don’t feel too convincing to you), but you do feel a little bit better. Maybe you feel more hope. In our client example, he put in row F an indication of his improved mental state: “More hopeful, less fearful.”
Once you’ve done the therapeutic work in rows D, E, and F, row G asks what you are going to go and do. It invites you to consider the question, “What is my responsibility to honor the new feelings I’ve created in row F?” From acceptance and commitment therapy we learn the principle that when we align our lives according to our most deeply held values, we experience improved mental health.[13] Discrepancies between our values and our behavior create greater emotional and behavioral dysfunction. And our mental health will continue to deteriorate the longer we are not acting in integrity according to our values. So row G is a way to say, “Okay, now that I’m looking at it in a healthier way, and I feel differently, what am I going to do about it?” You can put anything in this column that you feel is appropriate for your situation. Typically, clients are confused about what to do when they are anxious. Yet after completing this chart, they find that problem-solving can be easy. I have never had a client struggle to know what to put in row G after working through a thought chart. You can see that in our example, the client decided to “Let it go and move on and let the thought pass.” “Trust what I have written.” “Experiment and see if this works.”
Another client commented about the thought chart process: “I love [the] thought charts. These charts help ingrain healthy cognitive processes that breathe flexibility and contentment into my life.”
One Treatment Outcome Example, with Data
One client focused on this type of cognitive work in his therapy. He was a married man in his forties. He had been a long-term therapy client with many different therapists, but none were able to help him with his religious anxiety. He was so terrified that as I went into my waiting room to meet him for the first time, he had a panic attack right there! Here is part of his story:
I’ve had scrupulous inclinations for as long as I can remember. Even as a very young child, I never thought I was good enough. I wanted more than anything to live with God again, but I could never see myself as one of those people who would “make it” or “be saved.” For example, looking back, I can see the beginnings of what would become a fetish rooted in my early childhood years, and I knew without being told that I was dirty and unclean and outside God’s love.
When I was seven years old, my baptism was quickly approaching. I remember riding in the car, hoping that we would get into a fatal car accident before I turned eight. It wasn’t so much that I wanted to die, but more that I believed my religious tradition’s teachings that if I died before the age of eight, I would be guaranteed salvation. I “knew” with all my seven-year-old heart that I wasn’t going to be worthy of salvation if I lived beyond my eighth birthday.
Around eleven years of age, I was sexually assaulted by some slightly older kids in my neighborhood. The abuse continued over the course of the next year or so. One of the persistent challenges I had for many years was a belief that because I had experienced arousal, I was complicit in what had happened to me, adding yet another strike against my chance at salvation.
I had a father that had a severe chronic illness. When it came time to serve as a missionary in South America for my church, I didn’t know if my dad would be alive when I got home from my mission. However, while receiving a blessing to begin my missionary service, my ecclesiastical leader promised me that if I was faithful and obedient and a good missionary, then my dad would live to see me return from an honorable mission. What was intended as a message of hope instead became distorted in my mind. I inverted the intent of the promise. Any time I got a letter saying that my dad was getting sicker again, I wondered what I was doing wrong. My mind would begin cycling and ruminating through my behaviors of the previous weeks and wonder how my actions in this South American country were affecting my dad’s health in Utah. So I’d try to fix whatever I could. I believed that if my dad died, it was going to be my fault because I was not living up to my part of the promise. I believed I needed to be perfectly obedient or I’d cause my dad’s death. When I got news that my dad’s leg had to be amputated, it was like a physical slap in my face from God. I could feel His warning, telling me that I wasn’t doing enough. I believed my dad’s chance for life was directly correlated to every behavior of every moment. Every contact. Every lesson. Every conflict with my mission companion. Every study session. Every prayer. They all had to be perfect, or my dad would die. So much anxiety and guilt.
I started a slow downward spiral. There were ups. I got married. We had children. There were also downs. I could never accept myself, nor could I find any compassionate solace in my faith. I tried to be good and to serve, but nothing was ever enough.
After about five years of marriage, my mental health had degraded to the point that I was ready to end my life. I believed that my wife and kids would be better off if I weren’t around. But then my thinking shifted, and I started trying to figure out how I could take my family with me so I wouldn’t have to die alone. When I realized the horror of what I was considering, I finally realized that I needed to get help, immediately.
With the help of a psychiatrist, I found a moderately functional level of stability through medication, but it wasn’t enough. I started having panic attacks and irrational fears. During the course of the next decade, I met with several therapists who helped me with several other aspects of my mental illness, but any time we got near the scrupulous beliefs or the compulsive behavior linked to my fetish, I panicked. One time a counselor suggested I try to see myself as God sees me. I freaked out. Heaving sobs of panic and pain. My counselor instead suggested I try to see myself as my dad would see me (he’d passed away by that point). Again, I panicked. All I could think of coming from both God and my dad was this sentence: “You are such a disappointment.”
Then one day, I learned about scrupulosity. I felt a glimmer of hope.
As this man dedicated himself to his therapy process and mastered the thought chart and other skills, he learned to say to himself when he got triggered: “I have skills for this. What can I do to intervene before this cascades?”
It was rewarding for me to watch his journey over time as he learned to use the thought chart with success. Initially, he would have a heavily distorted row B thought and could not come up with disputes—his thinking just wasn’t very flexible because these fears had consumed him for so long. His wife (who joined us in the therapy sessions) and I initially needed to help him generate disputes. Shortly he began to learn how to create his own disputes. After months of practice, he could easily produce his own completed thought chart with a comprehensive dispute list in row D that would effectively bring down his distress.
As treatment continued, the way he talked in our psychotherapy sessions began to change. He would make a distorted, row B type of comment and then would follow it up with a “but” and then quickly rattle off several disputes. In time, as he continued to progress, his process shifted again—I would notice he would start to say a distorted row B thought, and then halfway through the thought he would interrupt himself to dispute it, never getting sucked into the negative emotion of it. And then his process changed again! At the end of his therapy treatment, he would dispute a thought even before saying it. He would notice that he was about to say a distorted thought and would catch it, recognize the distortion, and not even say it—without any negative emotional buy-in. He commented, “I’m not as rigid as I used to be.” After one year of cognitive therapy, he reported making more progress in that year than in ten previous years of therapy.
You can see in figure 11.4 an example of the type of thought chart he was able to produce near the end of his treatment process. In this chart he was working through a trigger from a religious meeting.
Figure 11.4. Client thought chart 2[14]
A | Activating Event |
|
B | Belief |
|
C | Consequences |
|
D | Dispute |
|
E | Eliminate |
|
F | New Feeling |
|
G | Go and Do! |
|
I assume the client took longer than thirty minutes on this chart based on the length of his dispute list, so I am not suggesting your dispute list needs to be this long, but I show you what he was able to produce on his own when he was in a healthier state so you can appreciate the absolute triumph of this process over his horrific scrupulous fears and anxiety! About the thought charts he said, “I learned that my thoughts are just thoughts, and I don’t have to believe them.”
His wife commented that he now had a different perspective in life. He was slower to react negatively, he intervened in the thought process earlier and could notice himself doing it (awareness), and when he did begin to struggle, he recovered more quickly.
Figure 11.5 shows charts generated by the Outcome Questionnaire 45.2[15] for this client over portions of his therapy process. This questionnaire is a general measure used for evaluating distress). As you can see, his distress significantly dropped over a year and a half of therapy.
Figure 11.5. Outcome Questionnaire-45.2 charts for client

The clinical cutoff score is represented by the dotted line at a score of 63, with an average score for a nonclinical, community population at 45. The first two charts show his first twenty therapy sessions. The third chart jumps ahead to show you his functioning from sessions 54 to 63. Our first session was a consultation only; therapy began six weeks later (marked as Session 2 on the chart). His increasing scores over the first nine sessions illustrate how his distress increased as he got closer to a major deadline at work but did not yet have adequate therapeutic tools to deal with the stress in a healthy manner.
You can see the sporadic nature of his distress during the first twenty therapy sessions. In the third chart, you can see that he had settled into a stable pattern of functioning, hovering right around the clinical cutoff score, with the majority of scores below the cutoff score. From there we continued to meet every three months or so for a while (beyond what is shown in these charts) to check in and maintain gains, and his scores continued to remain low.
As you can see, cognitive work is effective! While reflecting on his therapy journey, this client shared this perspective:
While there are therapeutic measures that show my progress, maybe my favorite measure is how my family sees me and responds to me. Just last week I reminded my seven-year-old how important it is to be flexible in her thinking, and she said, “That’s my dad!” I love that she sees me as a person who promotes flexible thinking in how we respond to life’s situations. After more than four years of avoiding temple worship (including while closed during the pandemic), I’ve recently returned, and I felt at peace. I’m able to think my way through most of my panic-inducing situations. I’ve even taken up some hobbies that include public performance, something inconceivable just a few years ago.
It’s been quite a journey. As I look back with compassion at my younger self, I wish I could let him know that help was on its way and that things would improve. I now understand that he was doing the best he could in the circumstances he was in. I did the best I could. I wasn’t perfect. But there is something beautiful to me in the dialectal beliefs that I wasn’t perfect, but I was doing the best I could, and it’s okay, and I was and am worthy of God’s love, and I can still grow and become better.
There is great power in trusting in the process. I’m so glad that I did. Two years ago, I was hiding in my bed, so depressed I couldn’t function. Today I’m happy, engaged in my life, and continuing to improve.
A caution: As helpful as the thought chart process can be, it is important to remember that with this and other cognitive techniques, you won’t be able to effectively do them or benefit much from them if you are doing them in the middle of an anxiety crisis, panic attack, or full-out meltdown. If you are out of your window of tolerance, then your cognitive skills tend to go offline. Do you remember the “battery incident” story shared by my client in chapter 1? In her story, my client reported that she stopped and did a thought chart in the middle of her crisis. The work she did is presented for you in figure 11.6.
Figure 11.6. Client thought chart 3[16]
A | Activating Event |
|
B | Belief |
|
C | Consequences |
|
D | Dispute |
|
E | Eliminate |
|
F | New Feeling |
|
G | Go and Do! |
|
I give this thoughtful client tremendous credit for being able to recognize in the moment that she was caught in an OCD crisis, but unfortunately, by the time she attempted the thought chart, her anxiety was simply too high—the anxiety swept her along and she ultimately found herself doing things she would typically never do in her futile efforts to assuage her anxiety. Can you see her battle in the chart (see her statements in the chart in parentheses)? She commented on this process, “Thought charts have been a significant part of my therapy process. They usually help to reduce my anxiety. I was dying for this thought chart to stop the madness, but I was still spiraling out of control. Looking back, I can see that my anxiety was so far outside my window of tolerance that the thought chart did little to reduce my anxiety. My brain’s fight/
Responsibility pie chart
As discussed in chapter 5, one of the main cognitive domains seen in OCD is “responsibility and threat estimation.”[17] Feeling overly responsible for everything and everyone fuels many obsessions and drives rumination. A responsibility pie chart can be very helpful in examining an inflated sense of responsibility.[18]
For example, a common concern for clients struggling with scrupulosity is a fear of getting someone sick or causing something bad to happen to another person. Generally, these people do not fear getting sick themselves, but the thought of getting someone else sick is terrifying. If this is you, you may feel your contribution to a potential feared outcome is the only factor contributing to the outcome (Did I wash my hands? Was I wearing a mask? Do I have any symptoms? = 100 percent of the responsibility for someone getting sick). This drives toxic anxiety and leads to a host of safety-seeking behaviors and compulsions.
Yet a responsibility pie chart can clarify for you that there is typically a variety of factors contributing to any potential feared outcome. This will help to challenge faulty assumptions and toxic guilt, teaching you that you just don’t have that much power!
Figure 11.7. Responsibility pie chart
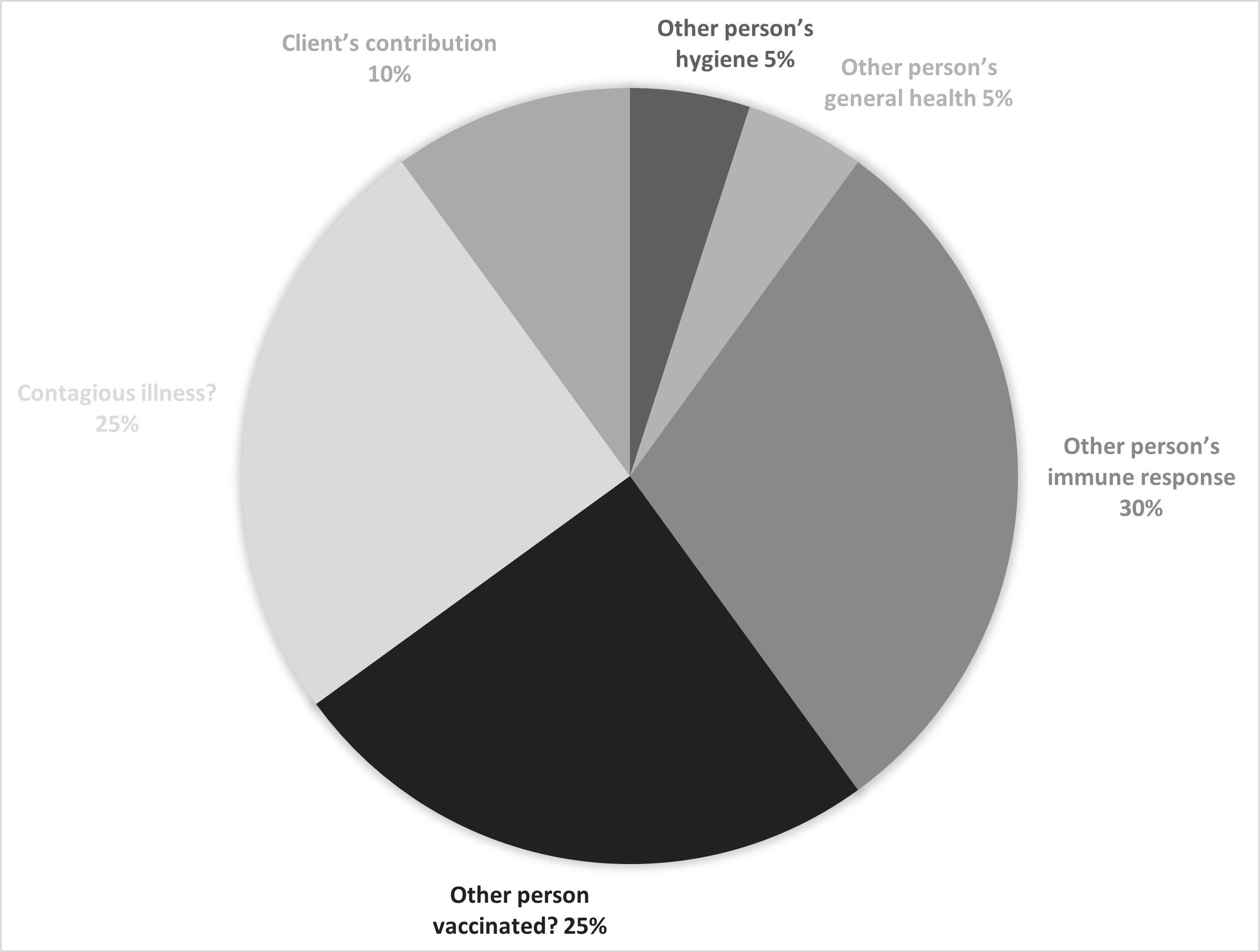
If you have this fear of getting someone sick and examine possible factors, as seen in figure 11.7, you might have to admit to yourself that the other person may genuinely have some influence on whether he or she gets sick or not. You may then begin to realize there may be several issues at play relative to that person’s contribution. List all the potential contributing factors and the probability of each factor contributing to the outcome. You might reason that whether someone gets sick or not may be affected by his or her own hygiene or handwashing behaviors (might account for 5 percent), general health (healthy/
Even though the numbers in the pie chart are just guesses, the main point of the exercise is to explore other factors that may share responsibility for a feared outcome’s possible occurrence. If you’ve believed the potential for a feared outcome is all on you (or mostly on you), realizing that you play only a small part in the total contributions to the outcome can shift your perspective quickly, helping you shed your excessive sense of responsibility and accompanying toxic guilt and rumination. It can facilitate a recognition of any cognitive distortions at play (such as all-or-nothing thinking, overgeneralization, jumping to conclusions, and so forth) and assist you in gaining a more reality-based perspective.
Transferring responsibility (to God)
Another cognitive responsibility technique you can utilize to ease scrupulous suffering is transferring responsibility for a potential feared outcome to someone else, including God. Researchers are finding that people who do this can reduce their OCD fears and anxiety stemming in part from an overinflated sense of responsibility.[19] However, this technique is not currently part of cognitive behavioral treatment protocols for three reasons. (1) Transferring responsibility to other people is not ideal because they are not always available or willing to assume responsibility. (2) Mental health professionals generally seek to assist clients in becoming more self-reliant rather than less so. (3) The other person’s own imperfections or humanity would be exploited by the OCD to undermine the transfer of responsibility in a manner that would be therapeutic. If you sought to employ this technique, you would need to be keenly aware that the other person has limited vision as a human being and cannot truly appreciate the risk due to the eternal weight, importance, and longevity of the scrupulous issues at hand.
However, God can be the appropriate recipient of that shift in responsibility, allowing devoted religious followers to tap into their faith to assist in their OCD treatment. God can be trusted to be omniscient—including knowing and understanding more about your scrupulosity than you even do. This is a positive way to transfer responsibility: give all obsessional fears completely and absolutely to God. It is not convincing yourself that bad things won’t happen to you or your loved ones, nor is it questioning the rationality of an obsessional fear as you would in a thought chart; rather, it is making a cognitive shift in your belief about who should take responsibility for it. This process is called a therapy of trust,[20] and it contains three steps:
- Recognize and identify obsessions when they strike. This principle is consistent with other therapeutic interventions for OCD discussed in chapter 10 on mindfulness and labeling anxiety.
- Transfer responsibility to God. Christians are familiar with the image of Jesus offered in the Bible: “Behold, I stand at the door and knock.”[21] “In the Therapy of Trust you invite Jesus into your life, share your horrifying, scrupulous fear with him, and then give him the responsibility for it. In essence, you are saying, ‘Here, Jesus, you look after this.’”[22] The cognition is that God will take responsibility for any fear you have, if you only turn to him with trust.[23] You can also see here the principle of acceptance.
- Prove your trust in God by resisting compulsions. Resisting compulsions diminishes frequency and intensity of intrusive thoughts and anxiety, but for religious believers it also proves their trust in God. Instead of performing compulsions, you can do some self-talk reminding yourself that it is more important to trust in God than to make certain that your fear does not come true. Putting your trust in God is pleasing to God. In this process you can grow closer to God while treating your OCD.[24] The Bible states, “But without faith it is impossible to please him: for he that cometh to God must believe that he is, and that he is a rewarder of them that diligently seek him.”[25]
This therapy of trust is compatible with cognitive-behavioral treatment protocols. It does not negatively impact exposure and response prevention’s emphasis on learning to tolerate uncertainty because transferring responsibility to God does so in a way that does not provide factual certainty. Doing your therapy is an act of faith. One of my clients, a widow in her sixties, found that this process truly helped give her courage to do some of her exposures:
Transferring responsibility for my OCD treatment to God was very helpful to me. Even with an unsettling exposure that was distasteful and abhorrent to me, my Heavenly Father knew it was therapy and I was going forward with the exposure process to try to get better. This helped me through the experience. Specifically, while performing sacred rites in our holy temple, I looped in my mind my fear of a specific act of disobedience, but I had faith and trust in God—that He understood my reason for such thoughts, and thus I wasn’t deeply wicked for such mental thinking. Trusting in God’s understanding of my OCD battles, and trusting in His priesthood promises of healing, has helped me on my path to healing.
Another client exercised this trust therapy by proxy, so to speak. She was serving as a missionary for The Church of Jesus Christ of Latter-day Saints and didn’t know what was happening to her emotionally. She felt like everything she did was breaking a law of God. She felt like she couldn’t trust herself. She did not feel worthy to be serving as a missionary (even though she was). Her mission president, who was also her ecclesiastical leader, did all he could to support her to be a successful missionary, including giving her access to a therapist and assisting her in obtaining OCD medication. She wanted to leave her mission and return home. The mission president asked her, “Do you believe I’m your priesthood leader?” To which she answered, “Yes.” He replied, in essence, “Your perceived sins are on me.[26] You are worthy to be here. Go serve your mission.” She had faith that her ecclesiastical leader was called of God, so she knew that what he said to her was true. She knew she could trust in his support, and she saw many miracles result from this newfound confidence. On this idea of transferring responsibility, she reported, “It is honestly how I got through.” She indicated that she couldn’t have completed her missionary service without that transfer of responsibility onto her trusted religious authority.
This concept of transferring responsibility to God can be a powerful concept for believers suffering with OCD. I look forward to additional research in this area.
Notes
[1] Abramowitz, J. S. (2018). Getting over OCD: A 10-step workbook for taking back your life (2nd ed.). Guilford Press, 146.
[2] Burns, D. (2006). When panic attacks: The new, drug-free anxiety therapy that can change your life. Morgan Road Books, 11–12.
[3] Burns, 2006. When panic attacks, 16.
[4] Linehan, M. M. (2015). DBT skills training handouts and worksheets (2nd ed.). Guilford Press, 50.
[5] Obsessive Compulsive Cognitions Working Group. (2003). Psychometric validation of the Obsessive Beliefs Questionnaire and the Interpretation of Intrusions Inventory: Part 1. Behaviour Research and Therapy, 41(8), (August 2003): 863–78; and Obsessive Compulsive Cognitions Working Group. (2005). Psychometric validation of the obsessive belief questionnaire and interpretation of intrusions inventory—Part 2: Factor analyses and testing of a brief version. Behaviour Research and Therapy, 43(11), 1527–1542. https://
[6] Burns, 2006. When panic attacks, 66–67.
[7] Grayson, J. (2014). Freedom from obsessive compulsive disorder: A personalized recovery program for living with uncertainty. Penguin Group, 115–117.
[8] Egan, S. J., Wade, T. D., Shafran, R., & Antony, M. M. (2016). Cognitive-behavioral treatment of perfectionism. Guilford Publications, 163.
[9] Egan et al., 2016. Cognitive-behavioral treatment of perfectionism, 164.
[10] Egan et al., 2016. Cognitive-behavioral treatment of perfectionism, 166.
[11] Burns, 2006. When panic attacks, 182.
[12] Client thought chart, used with permission.
[13] Hayes, S. C. (2005). Get out of your mind & into your life: The new acceptance and commitment therapy. New Harbinger Publications.
[14] Client thought chart, used with permission.
[15] Lambert, M. J., Gregersen, A. T., & Burlingame, G. M. (2004). The Outcome Questionnaire-45. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment: Instruments for adults (pp. 191–234). Lawrence Erlbaum Associates Publishers.
[16] Client thought chart, used with permission.
[17] Obsessive Compulsive Cognitions Working Group, 2003 and 2005. Psychometric validation of the Obsessive Belief Questionnaire, 863–878, 1527–1542, respectively.
[18] Veale, D. (1999). Cognitive therapy in the treatment of obsessive-compulsive disorder. Advances in Psychiatric Treatment, 5, 61–70; and Hyman, B. M., & Pedrick, C. (2010). The OCD workbook: Your guide to breaking free from obsessive-compulsive disorder (3rd ed.). New Harbinger Publications, 132–136.
[19] Shafran, R. (1997). The manipulation of responsibility in obsessive‐compulsive disorder. British Journal of Clinical Psychology, 36(3), 397–407. https://
[20] Osborn, I. (2008). Can Christianity cure obsessive-compulsive disorder? A psychiatrist explores the role of faith in treatment. Brazos Press, 161.
[21] Revelation 3:20.
[22] Osborn, 2008. Can Christianity cure obsessive-compulsive disorder?, 163.
[23] Osborn, 2008. Can Christianity cure obsessive-compulsive disorder?, 160.
[24] Bell, J. (2009). When in doubt, make belief: An OCD-inspired approach to living with uncertainty. New World Library, 116–120.
[25] Hebrews 11:6.
[26] Jacob 1:18–19 helps us understand how priesthood leaders have stewardship for those they serve: “For I, Jacob, and my brother Joseph had been consecrated priests and teachers of this people, by the hand of Nephi. And we did magnify our office unto the Lord, taking upon us the responsibility, answering the sins of the people upon our own heads if we did not teach them the word of God with all diligence; wherefore, by laboring with our might their blood might not come upon our garments; otherwise their blood would come upon our garments, and we would not be found spotless at the last day.”
