Behavioral Features in the Development and Maintenance of Scrupulosity
Debra Theobald McClendon, "Behavioral Features in the Development and Maintenance of Scrupulosity," in Freedom From Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Provo, UT: Religious Studies Center, Brigham Young University; Salt Lake City: Deseret Book), 79–94.
Behavioral features in the development and maintenance of scrupulosity generally coalesce around a person’s compulsions and avoidance behaviors. As we have discussed, people perform rituals that may be common in their religious community, but the rituals are generally done in an extreme, compulsive fashion. Behaviors associated with prayer, confession, fasting, or other religious rituals may be done excessively, driven by pathological guilt and anxiety. Other safety behaviors, such as avoidance or suicidal ideation or gestures, may also be involved in neutralizing anxiety. Researchers have commented, “OCD sufferers may initially be seeking to be scrupulous (in a nonpathological sense), but the problem grows until functioning is severely affected. The initial concern was appropriate, the eventual consequences destructive.”[1]
Safety Behaviors
Safety behaviors, or safety-seeking behaviors, are overt or covert maladaptive coping behaviors used to reduce anxiety and fear when you feel threatened.[2] They are any mental or physical actions taken to suppress or neutralize intrusive or obsessional thoughts, diminish anxiety, gain reassurance, or prevent feared consequences.[3]
“Many safety-seeking behaviors are helpful and adaptive when the concern is real and the behavior can genuinely reduce the danger, such as checking the temperature of the water before getting in the bath or looking both ways before crossing the road. However, when safety-seeking behaviors concern perceived threats rather than actual dangers they are either unnecessary or can serve to exacerbate and maintain the anxiety.”[4] In the struggle with scrupulosity, the anxiety is getting triggered in the absence of actual threat.
Safety behaviors, when used in response to perceived threats (rather than responding accurately to actual danger), include compulsions, but it is a broader category not limited only to compulsions. Safety behaviors can also include not looking at certain people or certain things, not listening to certain music, instructing others not to discuss certain topics around you, or proscribing certain behaviors to others, such as giving them rules to follow to avoid triggering your anxiety.
Some examples of safety behaviors specific to scrupulosity include excessive praying, repetitive confessions, avoidance of scripture study or attendance at religious meetings, or the performance of compulsions. Some examples of safety behaviors that could be seen in both scrupulosity and social anxiety include avoiding church or other meetings, sitting in the back of church meetings to be able to make an early or easy escape, sitting in the lobby to avoid the main meeting room, avoiding eye contact, avoiding talking to people, turning down invitations to activities, leaving church when a triggering topic comes up, avoiding or procrastinating working on church duties, avoiding prayer or scripture study or other personal worship activities, or even turning down assignments (i.e., “callings”).
Compulsions
Compulsions, or rituals, do work temporarily to reduce anxiety, so those with scrupulosity will use them when their anxiety is high to get any tiny bit of relief. However, those that suffer with scrupulosity would admit, when pressed, that their compulsions are not actually solving their anxiety problem long term (or why else would they still need to do them?).
Five reasons why compulsions don’t work[5] include the following:
- When performing rituals, you believe the lack of a bad outcome is a result of having done the ritual. You are not able to falsify your false beliefs, so you don’t end up learning that the compulsion is actually useless and senseless.
- Compulsions interfere with your ability to learn that you can tolerate obsessions, anxiety, fear, uncertainty, and other undesirable experiences. Instead, you come to believe that you cannot live a meaningful, valued life if these are present.
- Since the compulsions sometimes lead to an immediate reduction in anxiety, you want to do them again and again because nothing else has seemed to work at all. However, since the relief you feel is only temporary, you have to keep going back to the compulsions again and again and again—they don’t end up solving your problem.
- As you continue to return to your compulsions, over time the dysfunction increases. Rituals end up growing more complex over time, taking more of your time and energy. This interferes with daily functioning. The rituals stop providing the temporary relief you expect.
- The more compulsions you perform, the more you are reminded of your obsessional fears. You think about them more! And so, the more your anxiety is triggered and you continue to turn to the rituals.
One particularly compelling compulsion for scrupulosity clients is reassurance seeking, discussed previously. Researchers found that people with scrupulosity who exhibited reassurance-seeking behaviors had more severe obsessions than their peers who did not rely on such behaviors, suggesting that reassurance seeking plays a role as an additional coping strategy when obsessions are more prominent.[6] So when you find yourself reassurance seeking, remember that it is not an adaptive coping strategy; it ends up causing more problems than it resolves—and will ultimately keep you trapped in the obsessive-compulsive cycle.
Avoidance
The belief that you can safety seek through avoidance is another lie perpetuated by anxiety. It tells you: flee, run, avoid, don’t look, don’t go! Yet avoidance doesn’t solve your problem and keeps you trapped, perpetuating a vicious cycle of toxic anxiety. Here are four reasons why avoidance doesn’t work[7] to assuage anxiety:
- Avoidance doesn’t work because you will only be successful at avoiding a feared stimulus for so long—eventually you’ll encounter something you can’t avoid, and then it will trigger obsessions, anxiety, and even panic.
- Avoidance prevents you from learning that your feared stimulus (object or situation) is not really dangerous because you don’t allow yourself the opportunity to confront it. You will remain anxious.
- Avoidance interferes with your ability to learn that your intrusive thoughts, obsessions, or other unwanted internal experiences aren’t harmful and that you can learn to tolerate them.
- Trying to avoid every possible anxiety trigger will shut your life down—you will continually become more restricted as the OCD rules overgeneralize and get more limiting as you seek to “guarantee” safety.
Safety behaviors aren’t safe
When you have poorly regulated anxiety, so-called safety behaviors such as compulsions, reassurance seeking, and avoidance aren’t safe. They’re not helpful. They are not going to successfully help you to resolve anxiety, and in the end they create greater anxiety: safety behaviors “become maladaptive over the long term by prolonging anxiety and fear of nonthreatening situations.”[8] They make your situation worse because the anxiety starts to get overgeneralized to other areas that were previously not anxiety provoking! Then the anxiety continues to get progressively worse. It is so difficult because you’re suffering and don’t know what else to do that will work, and these safety behaviors have at least reduced anxiety on some level previously, so you chooseto do it again, and then do it again. You get stuck; you know you are trapped.
So don’t make following anxiety’s demands a priority. Anxiety is uncomfortable—it’s horribly uncomfortable—but it is not dangerous or harmful. Also, the anxiety won’t last forever; it’s temporary. In fact, it will even eventually decrease on its own if you leave it to go through its own natural process (rather than trying to control it with safety behaviors like compulsions). This is an especially important principle for anyone struggling with anxiety, but particularly for those of you with scrupulosity OCD. You don’t have to do anything to make the anxiety go away, even if you are still in the anxiety-producing situation or being exposed to the anxiety-producing stimulus. That is the main principle behind exposure treatment, which we will talk about in part 3 on treatment.
The Vicious Cycle of Anxiety
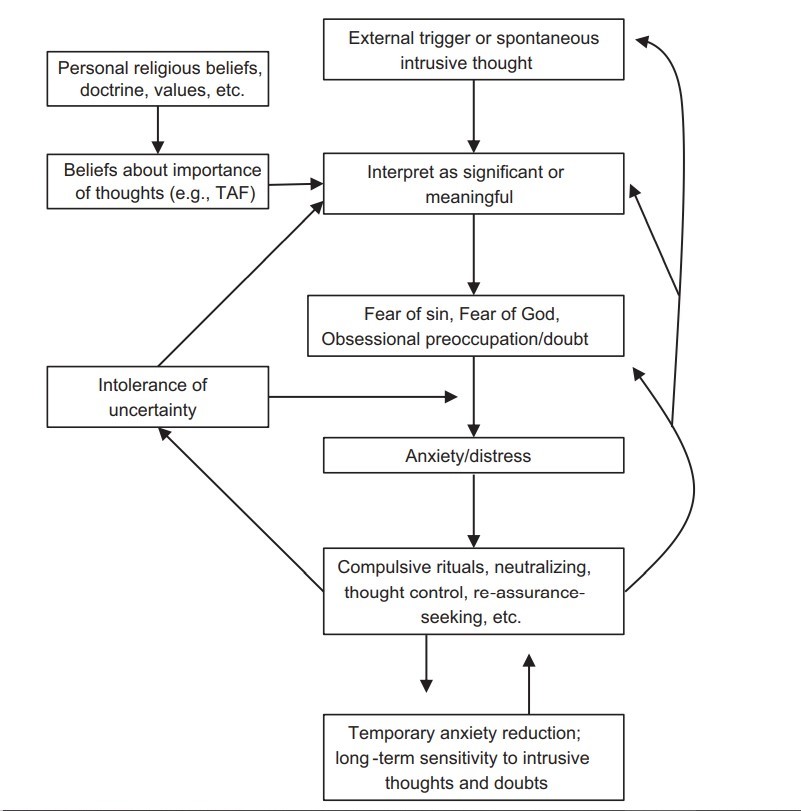 Figure 6.1. The vicious cycle of anxiety[9]
Figure 6.1. The vicious cycle of anxiety[9]
Figure 6.1 broadly illustrates the vicious cycle of anxiety as seen in anxiety disorders and OCD. If we look at the top of the chart, you begin with experiencing anxiety; then, following the arrow to the right, you have increased scanning for danger. As you’re hypervigilant for possible threats, your physical symptoms of anxiety intensify. Your attention narrows and focuses more fully on yourself because the anxiety feels so bad—because you’re feeling so bad. This leads to escape or avoidance safety behaviors because you’re trying to do anything you can to reduce the discomfort of the anxiety. As I mentioned, safety behaviors do work, but only temporarily for the short run. In the long term, you’ll experience an increase in the physical symptoms.
In addition, when you give in to the urge to escape or avoid, you’ll experience a loss of confidence in your ability to cope with your own life circumstances, or to cope with your own anxiety or emotions. This is one of the biggest consequences that I see in my clients who give in to the compulsive cycle. I have very bright, intelligent, hardworking people who come to see me because of their struggle with scrupulosity. And yet these highly competent individuals have lost confidence in their ability to handle their lives and their emotional landscape. It’s devastatingly sad for them because they can see and feel the dramatic negative changes in themselves brought about by the compulsive cycle. Obviously, the loss of confidence impairs their ability to function in their lives. Have you noticed this consequence in your life?
So, again on the chart, with that loss of confidence you will have an increased use of safety behaviors to try to neutralize your anxiety. But they only lead to more anxiety in the long term and you’re back to the top of that chart. The obsessive-compulsive cycle goes around again and again and again.
Cognitive-Behavioral Model of Scrupulosity
More specifically, researchers have applied a cognitive-behavioral model of obsessional problems to describe the development and maintenance of scrupulosity. This model, as seen in figure 6.2, emphasizes, as discussed in chapter 5, how obsessions are influenced by maladaptive beliefs and misinterpretations of unwanted, distressing thoughts (that are actually normal and universal),[10] while also showing how behavioral features like compulsions affect the process.
This conceptualization also addresses the influence of religious doctrine, including the recognition that important aspects of religion are not subject to certainty or objective verification—they must be taken on faith. As the person suffering with scrupulosity tries to gain a sense of certainty (i.e., assurances) and to control intrusive thoughts and doubts, his or her efforts paradoxically, and unfortunately, set in motion a self-perpetuating, vicious obsessive-compulsive cycle.[11]
Does this examination of these behavioral features imply that your OCD is your fault?
No. This is not to blame scrupulosity sufferers for their own misery. Many with scrupulosity are harsh with themselves, imposing blame for the affliction. If this is you, consider this encouraging perspective:
Is there truly any justification for blaming yourself that you have panic attacks, phobias, or obsessions and compulsions? Is it truly your fault that you developed these problems? Is it not more accurate to say that you’ve done the best you could in your life up to now with the knowledge and resources at your disposal? While it’s up to you to change your condition, there is simply no basis for judging or blaming yourself for having it.[12]
Figure 6.2 Cognitive-behavioral model of scrupulosity[13] (“TAF” in this chart refers to thought-action fusion, to be discussed in chapter 7.)
Indeed, one researcher points out three parts of this vicious cycle that are involuntary:[14](1) the occurrence of intrusive thoughts, (2) anxiety and the automatic trigger of the fight-or-flight response when you encounter a feared stimulus, and (3) the fact that compulsions and avoidance used to try to soothe and diminish intrusive thoughts end up making things worse over time.
However, it doesn’t mean that you can’t do something to help yourself. There are two elements of this vicious cycle that are voluntary[15]—these are within your control: (1) your interpretation and response to unwanted, distressing intrusive thoughts, and (2) whether you choose to use compulsions and avoidance in response to your anxiety. You can do something to interrupt this cycle. You won’t be successful intervening at the level of the involuntary elements, but you can intervene with those responses that are within your voluntary control. This is the work of OCD treatment—to learn to accurately interpret these thoughts as nonthreatening, as well as learn to choose new behavioral responses to obsessional fears.
Suicidality
The potential for self-harm or suicide is a serious concern. In this section I cover suicidality’s interplay with OCD. I offer definitions and discussion about suicide in the United States and suicide in OCD in general. Then I explore how suicide takes on a particular flavor in scrupulosity.
OCD obsessions can present as suicidal thoughts. People suffering with OCD, especially self-harm OCD, may be afraid they will act on their suicidal thoughts, but they are not severely depressed and do not wish to die. The obsessional suicidal thoughts are ego-dystonic (they are in conflict or dissonant with one’s sense of self). Once you identify that the suicidal thoughts are obsessions rather than a true manifestation of desire, they are treated the same way other OCD symptoms are treated.[16]
However, true suicidal thought is not ego-dystonic, but ego-syntonic (compatible with one’s sense of ego), resulting from severe depression. Suicidal ideation is thinking about or considering suicide or being preoccupied with death and suicide. This is typically not a serious consideration of suicide. It is generally an “escape fantasy.” The escape fantasy constitutes the ultimate avoidance and safety behavior. The person with suicidal ideation wants to escape the anxiety, torment, and pain. For example, when I discuss suicidality with clients, most frequently they say, “I think about it, but I would never do it.” A suicidal plan is when someone has chosen details for how to act on suicidal thoughts. Someone with suicidal intent has a plan that outlines how to enact suicide and has secured the means available to execute that plan. For example, if someone has a plan to overdose on a medication, intent is shown by gathering or hoarding the pills so they are available for ingesting at any chosen moment. A suicidal attempt is when someone enacts a plan with the intent to die, but the attempt turns out to be nonfatal. A suicide or completed suicide or death by suicide is a death caused by self-directed injurious behavior with the intent to die as a result of that behavior.
As you examine these definitions, you can see that as someone moves from passive suicidal ideation to more proactively thinking about creating a plan and carrying out that plan, the situation is increasingly more serious relative to the intensity of distress and the deterioration of the person’s mental health and resilience. Furthermore, things are becoming more dangerous as well. This type of shift in thinking should always be taken seriously. To maintain safety, please seek mental health treatment if you are not currently in therapy or do not choose to discuss the suicidality with your therapist if you are currently in treatment. If at any time you (or a loved one) are in suicidal crisis, please go the emergency room at your local hospital or call 911. This book is not sufficient as a sole therapeutic resource if you are in a suicidal crisis.
Now let’s look at suicide specifically in obsessive-compulsive disorder. Rates of suicide are generally higher for those with OCD than for the general population. In a comprehensive study done in Sweden with its national registers, researchers[17] found that those with OCD are at risk of dying by suicide ten times more than the regular population. The risk of attempted suicide is five times higher than it is for the general population. This study also found that the risk of dying by suicide was more pronounced in the women with OCD. Women also had higher rates of suicide attempts. Those with OCD that had previously been admitted to the hospital as inpatients also had a significantly higher risk of suicide and higher risk of suicide attempts than did those who were outpatients.
For those with OCD, a previous suicide attempt was the strongest predictor of a completed suicide—32.84 percent of those that died by suicide had a recorded previous suicide attempt. In fact, it gave them an increased risk by five times. In addition, having a comorbid (co-occurring) personality or substance use disorder increases the risk by about 90 percent. The majority of completed suicides involve some sort of substance abuse as well.
Researchers identified specific risk of suicide rates by those suffering with specific symptomology: contamination and cleanliness (57 percent), religious obsessions (45 percent), sexual obsessions (33 percent), repeating rituals (31 percent), and other obsessions (27 percent).[18]
Choice of suicidal means is important to be conscientious of because some means (such as drug ingestion) may create buffer time to save a loved one, whereas some means (such as the use of firearms) do not. It’s interesting to note that in OCD, self-poisoning seems to be the most frequently used method of attempting suicide. Researchers found that patients with OCD are less likely to use violent methods of suicide. This may be consistent with the personality profile of this patient group, described as being harm avoidant.[19] The researchers additionally speculated that since 85 percent of their sample were using psychotropic medications for their OCD, it may be possible that self-poisoning was chosen due to the convenient access to medications.
How does suicide look specifically in scrupulosity OCD? For one client struggling with scrupulosity, depression, and suicidal ideation, the distress led him to think, “Suicide will stop me from sinning or making mistakes in mortality.” Yet religious belief is generally a protective factor against suicide. For example, this client believed, “Suicide is a sin in itself, a very grievous one.” “We don’t know much about the penalty for suicide, but there is one and it is a sin.” However, one researcher has said that those who suffer from severe and long-term scrupulosity may ironically surrender to the “urge to commit the sin,”[20] a strong indicator of severe distress and hopelessness. They may, because of their religious belief, believe that committing suicide is a sin but in the end choose to give up. The potential for self-harm and suicide resulting from these types of feelings of desperation and hopelessness is always a concern. Please be wise in this area.
Following are some comments from people that are either struggling with or have recovered from scrupulosity so that you can see some different flavors of suicidal ideation in scrupulosity. These first two comment that their religious beliefs influenced their view of suicidality. However, on a conscious level, suicidality never entered their minds.
- “Suicide never entered my mind. It wasn’t an option because of my religious beliefs, as well as the culture at the time. My struggle was twenty years ago, and the culture of suicide at the time was very different. It just wasn’t seen as an option.”
- “I don’t remember having suicidal thoughts or feelings at the time I was going through the worst of my scrupulosity. It may be because of the scrupulosity itself always being ruled by the morality of things. Maybe feeling that suicide was wrong and would lead to damnation was one reason it never entered my mind, even with the degree to which I was suffering.”
So there may be some people for whom suicidal ideation is just not of concern. You will want to be wise if you are a family member or friend, ecclesiastical leader, or a treatment provider. You’ll want to ask people how they feel and what their thoughts are about this so you can do what you can to help maintain safety.
- At the darkest point of my suicidality, I struggled a lot with suicidal issues. The only thing that mattered was to be worthy, and in my head, I could not get there. I wished that I could die so that I could talk with Heavenly Father myself and work out my worthiness with him. I also believed that I had done so much evil in my life that I was going to be permanently unclean, that I would not be able to accomplish any of my dreams, such as a temple marriage and a happy life. I felt that I had ruined my life. And I was in such immense emotional pain that I wanted to give up through suicide. I eventually was able to meet with a counselor and learn that my thoughts were not reasonable and was able to see myself through more reasonable lenses. It didn’t get better quickly and is still a battle. But I was able to learn to accept the uncertainty of KNOWING if I was worthy or not, and had to have faith that I was, or could be, and then continue forward.
- In the darkest moments of scrupulosity—when my mind is racing with intrusive thoughts, when guilt becomes almost unbearable, and when anxiety escalates to raw terror, the thought of death, or simply being banished from existence, is often one of the only solaces I have left. Cancer, or any other terminal illness, can feel welcome at those times because the spiritual and mental pain are so intense that I would trade them for almost anything. As a Christian, I try to remember that the Savior has felt exactly what I have felt, and he is always there, even when I cannot see him or feel him. I always try to remember there are other ways to see his hand and evidence of his love outside of feelings alone, and his support may actually come through others. There’s a Swedish proverb that says, “Shared joy is a double joy; shared sorrow is half sorrow,” and I believe it. Sharing my burdens with others lightens them and illuminates some of the darkness, and sharing my joys with others reminds me of the things that make life on this planet worth living.
- I was in a scrupulosity crisis about three years ago. I had been stuck in a horrible thought spiral and had felt rather depressed. I was sitting in the celestial room in the Salt Lake Temple when a random brother walked up to me and said, “This message is for you: Don’t ever give up.” Two years later, I was in the worst scrupulosity crisis of my life and was coming to understand on a deeper level why some people choose to take their own life. The emotional pain I was enduring was absolutely crushing and fatiguing. I remember thinking at my lowest of lows that I didn’t think I could make it even another week, yet for whatever reason I knew suicide was not the answer. Looking back, I have come to realize that the Lord knew I would struggle immensely with scrupulosity, which is why I had that directed message given to me during a scrupulosity crisis. That experience in the temple was a rock for me, that has helped me endure unbearable pain until help finally arrived. And help did come, and pain has been replaced with joy.
For those of you who personally know the type of pain these people are describing, the pain that torments you can be replaced with joy as you seek healing and engage in the necessary treatment interventions. Please make a commitment to stay safe, and if you feel like you cannot maintain that commitment, please seek out appropriate intervention to maintain safety.
Notes
[1] Greenberg, D., & Huppert, J. D. (2010). Scrupulosity: A unique subtype of obsessive-compulsive disorder. Current Psychiatry Reports, 12, 285.
[2] Safety behaviors (anxiety). (n.d.). In Wikipedia. https://
[3] Abramowitz, J. S. (2005). Understanding and treating obsessive-compulsive disorder: A cognitive-behavioral approach. Lawrence Erlbaum.
[4] Psychology Tools. (n.d.). Safety-Seeking Behaviors / Safety Behaviors. https://
[5] Abramowitz, J. S. (2018). Getting over OCD: A 10-step workbook for taking back your life (2nd ed.). The Guilford Press, 79–81.
[6] Starcevic, V., Berle, D., Brakoulias, V., et al. (2012). Interpersonal reassurance seeking in obsessive-compulsive disorder and its relationship with checking compulsions. Psychiatry Research, 200(2–3), 560–567.
[7] Abramowitz, 2018. Getting over OCD, 81–82.
[8] Safety behaviors (anxiety). (n.d.). In Wikipedia.
[9] Centre for Clinical Interventions. Anxiety—Reversing the vicious cycle. https://
[10] Abramowitz, J. S., & Jacoby, R. J. (2014). Scrupulosity: A cognitive-behavioral analysis and implications for treatment. Journal of Obsessive-Compulsive and Related Disorders, 3(2), 142.
[11] Abramowitz & Jacoby, 2014). Scrupulosity, 143.
[12] Abramowitz & Jacoby, 2014. Scrupulosity, 142.
[13] Bourne, E. J. (2020). The anxiety and phobia workbook. New Harbinger Publications. Kindle Edition, 83.
[14] Abramowitz, 2018. Getting over OCD, 83–84.
[15] Abramowitz, 2018. Getting over OCD, 83–84.
[16] Shapiro, L. J. (2020). Obsessive compulsive disorder: Elements, history, treatments, and research. Praeger, 144.
[17] Fernández de la Cruz, L. et al. (2017). Suicide in obsessive-compulsive disorder: A population-based study of 36,788 Swedish patients. Molecular Psychiatry, 22, 1626–1632. https://
[18] Shapiro, 2020. Obsessive Compulsive Disorder, 144.
[19] de la Cruz et al., 2017. Suicide in obsessive-compulsive disorder, 1626–1632.
[20] Ciarrocchi, J. W. (1995). The doubting disease: Help for scrupulosity and religious compulsions. Paulist Press, 36.
