Anxious, Anyone?
Debra Theobald McClendon, "Anxious, Anyone?," in Freedom From Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Provo, UT: Religious Studies Center, Brigham Young University; Salt Lake City: Deseret Book), 1–18.
Part I: Leading into Scrupulosity: The Basics
In part 1, chapters 1 through 3, I lay out some foundational concepts important to understanding obsessive-compulsive disorder (OCD) generally and scrupulosity specifically. These chapters will set the stage for getting into more complex scrupulosity issues in part 2 and exploring treatment in part 3. Here is a road map for you so you can anticipate what you’ll encounter in part 1.
In chapter 1, “Anxious, Anyone?,” I discuss basic characteristics of anxiety and how normal, nonpathological anxiety can be helpful to us in our lives. I explore how you can discern between normal levels of anxiety and an anxiety disorder. I then present the diagnostic criteria for OCD and briefly explore obsessions, compulsions, and reassurance-seeking rituals.
In chapter 2, “Anxiety versus the Spirit,” I discuss how moderate and high levels of anxiety interact with spiritual communication. I discuss how anxiety and the Spirit tend to communicate differently, including presenting a chart I constructed with clients that contrasts some feelings of anxiety and feelings of the Spirit. I show some additional “anxiety versus the Spirit” charts that clients put together during their therapy process. I hope these charts will encourage you and stimulate thoughts about your own experiences. At the end of the chapter, I discuss why understanding the differences in how the Spirit and anxiety communicate is critical to pursuing the correct therapeutic path.
In chapter 3, “Intrusive Thoughts,” I discuss the nature of intrusive thoughts. I contrast the differences between how those without OCD and those with OCD respond to intrusive thoughts. I define varying thought processes. Lastly, I introduce scrupulosity, the primary focus of the remaining chapters. I conclude the chapter by answering the intriguing question, “Is my scrupulosity caused by Satan?”
Chapter 1
Anxious, Anyone?
Anxiety is ubiquitous, and it lies at the core of scrupulosity. Understanding the basic nature of anxiety is helpful to understanding more fully how and why scrupulosity operates in the lives of people in the complex manner that it does.
What is anxiety? Anxiety is a state of excessive uneasiness and apprehension about something that is planned or might happen in everyday situations. It may feel like worry, fear, or dread. The symptoms of anxiety often include nervousness, difficulty concentrating, nausea, rapid heartbeat, panic, muscle tension, sleeping problems, and so on.
Anxiety is typically future-oriented, associated with “vigilance in preparation for future danger and cautious and avoidant behaviors.”[1] It is the emotional reaction we have in anticipation of a future danger, threat, or trouble. The uncomfortable symptoms of anxiety come to you to help you prepare for future danger, although anxiety can also be generated when ruminating, or thinking obsessively, about past experiences.
Anxiety Is Normative and Can Be Helpful
Anxiety is normative. It’s a normal emotion—just like happiness, joy, anger, grief, or sadness. Anxiety gives us information, such as if we need to prepare to respond to an event. Since anxiety is an uncomfortable emotion, you might be tempted to try to make a therapeutic goal to get rid of your anxiety. Although high levels of anxiety are miserable and damaging to one’s life, moderate levels of anxiety can be well tolerated and are actually adaptive, helping to improve our performance—so don’t try to get rid of all of it. We are benefitted by a healthy dose of anxiety in our lives! Anxiety helps us to anticipate and prepare by focusing our attention on only what is necessary.
Spend a moment to ponder how anxiety may have helped you in the past. If you think about presentations, lessons, talks, or sermons in church that you have given, can you see how some concern anticipating the event blessed you to give a better presentation? Or perhaps at some point in your life you’ve had to prepare for exams in school or other performances, such as a musical or theatrical performance. If we use a student example, chances are that if you didn’t have some nervousness or anxiety about doing well in school, you might not have studied and prepared much for tests. Certainly, failing to study adequately for an exam doesn’t tend to produce highly desirable scores, so a low level of anxiety is actually not the ideal. A moderate level of anxiety that motivates you to prepare more thoroughly is helpful in performing at an optimal level.
However, be aware that anxiety can be problematic at higher levels. In fact, anxiety impairs performance at these levels. If you look at figure 1.1,[2] you’ll see a presentation of the Yerkes-Dodson Law.[3] This model has been used to explain the relationship between constructs such as pressure, anxiety, stress, tension, arousal, and performance. It shows that performance increases with mental or physical arousal, but only up to a point.
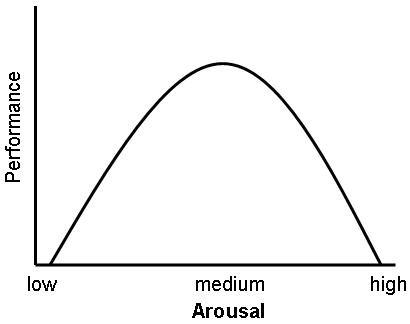 Figure 1.1. Yerkes-Dodson Law: Inverted U-relationship between arousal and performance
Figure 1.1. Yerkes-Dodson Law: Inverted U-relationship between arousal and performance
You’ll see that low anxiety produces lower performance efficiency. When you are underaroused you tend to get bored and not perform as well. Yet as anxiety increases to a moderate level, performance efficiency increases. The moderate level of anxiety produces an optimal level of performance.
However, as you move to higher levels of anxiety, your performance drops. Have you ever bombed a test that you had studied for because you were so nervous you couldn’t recall the information, even though you knew you knew it? Have you ever choked in a piano recital or fallen off the balance beam in a gymnastics competition? We’ve probably all had that kind of experience. When anxiety is too high, one’s experience may be panic, tears, numbing out or going blank, a full-on emotional meltdown, or even toxic guilt (in contrast to legitimate guilt in response to sin).[4]
This dynamic can be understood from the concept of flow. If an activity is not challenging enough, we get bored. If the challenge overwhelms our skill level, we get anxious or frustrated. (Anxiety in this situation is a clue that we need to work to build proficiency or alter the activity to fit our skill level.) However, in flow we are absorbed in what we are doing, and we have successfully balanced our skills with our challenges. In flow our experience “falls in just the right space between boredom and anxiety.”[5]
One insightful woman found this to be an important point for her. When performing piano solos in church, she tended to choose extremely difficult music that showed off her impressive skill but stressed her out, so the process of preparing and giving the performance was not enjoyable. She found that if she cut back slightly on the difficulty level of the music, the music would still be a beautiful worship offering for others and she could also enjoy the process of sharing her talents in praise of her God.[6]
What Is an Anxiety Disorder?
If anxiety is normal, and everyone has it at various times to one degree or another, then how do you identify when anxiety has become a problem—an anxiety disorder? In general, mental illness is the presence of all three of the following elements: dysfunction, distress, and an atypical cultural response.[7]
A psychological dysfunction refers to a breakdown of normal functioning in the cognitive, emotional, or behavioral processes. Experiencing uncontrollable crying and grief, restricted emotional reactions (i.e., appearing to have only one emotion, such as anger), memory problems, chronic fear when situations are nonthreatening, and such are all examples of a psychological dysfunction. Compulsive behaviors or activities may dominate life so there is no time or mental space for meaningful interactions and relationships with loved ones.
Personal distress is also a factor in defining mental illness and generally accompanies the breakdown in functioning. People may suffer from a host of symptoms throughout their lives for which they may never seek treatment because the symptoms are just a transient part of normal life and nothing to worry too much about (such as an occasional headache or nervousness before trying something new). A common psychological maxim says, “Normal is not symptom free.” For example, it is possible to have an isolated panic attack that does not lead to continued anxiety problems. In this case there would not be a panic disorder diagnosis, because the person is not experiencing ongoing distress.
If there is distress there is a problem. The symptoms that cause us a great deal of concern are the ones that take us to a doctor to seek a diagnosis in hopes of getting treatment. In the panic attack example, when a person has had a panic attack and is very distressed about it, he or she may begin to worry excessively about having another panic attack. With that worry the person may then begin to alter and restrict certain activities and thoughts according to that fear. That type of distress contributes to the possible diagnosis of a panic disorder.
Every disorder has its own flavor of distress. While depression may be very dark and bleak, anxiety tends to be miserably unsettling, pressuring, and chaotic. While those with various disorders all experience distress differently, generally they hate how they feel and what they are doing, but are paralyzed and stuck, not knowing how to change it because of the severity of their dysfunction.
In defining mental illness, it also becomes important to evaluate if it is an atypical cultural response, one not typical within the culture. Even if there is dysfunction and distress, if the person’s experience is just like everybody else’s, a diagnosis at that point would become meaningless. In contrast, the problem is atypical or not culturally expected if it is a deviation from the norm. Generally, most psychological disorders have a prevalence rate of 1 percent, meaning that only one person out of one hundred people has this problem. This represents an atypical cultural response. However, the problem may also be considered atypical for one’s culture if it is a severe violation of social norms.
Scrupulosity Is a Form of OCD
Although anxiety is a normal emotion that serves a variety of adaptive purposes, indeed, more serious problems come if the anxiety persists, feels uncomfortable or overwhelming, and begins to interfere with daily activities. In OCD, anxiety takes on an extreme, destructive nature. This is different from anxiety experienced during normal, everyday living or even perfectionism. Let’s take a closer look at OCD.
Some OCD statistics
Since OCD is a mental illness, it affects a small number of people relative to the general population. In the United States, the twelve-month prevalence rate, the percentage of the population that has OCD at any given point in a twelve-month period, is about 1.2 percent. A similar prevalence rate is seen internationally (1.1 percent–1.8 percent);[8] prevalence rates do not vary much across cultures.[9] However, a larger proportion of people may have OCD-like symptoms without receiving a formal diagnosis.
In the United States, the average age of onset is nineteen and a half years, with a significant number of cases (25 percent) starting before age fourteen. Onset after age thirty-five is unusual. There are some gender differences in age of onset, with males typically having an earlier age of onset than females (almost 25 percent of males have onset in childhood before age ten).[10] Those with OCD frequently struggle with depression as well.[11]
The perinatal period is a risk factor for the onset or exacerbation of OCD.[12] Pregnant women and postpartum women are more likely to experience OCD one and a half to two times more than the general population. Specifically, this risk is higher for those in the postpartum period than for those during pregnancy. For example, the prevalence rate of OCD during pregnancy ranges from 0.2 percent to 3.5 percent, while the prevalence of OCD during the postpartum period ranges from 2.7 percent to 9 percent.
OCD diagnostic criteria
The Diagnostic Statistical Manual, fifth edition (DSM-5), is the handbook for mental health professionals that catalogs psychological disorders and provides diagnostic criteria for identifying and diagnosing the disorders. The DSM-5 presents a chapter on anxiety disorders and then follows it with a separate chapter on obsessive-compulsive and related disorders, which include not only OCD but also body dysmorphic disorder, hoarding disorder, trichotillomania (hair-pulling disorder), excoriation (skin-picking) disorder, and the like. It indicates “there are close relationships between the anxiety disorders and some of the obsessive-compulsive and related disorders (e.g., OCD), which is reflected in the sequence of the DSM-5 chapters, with obsessive-compulsive and related disorders following anxiety disorders.”[13]
The DSM-5 states that OCD differs “from developmentally normative preoccupations and rituals by being excessive or persisting beyond developmentally appropriate periods.”[14]
Scrupulosity OCD manifests itself in obsessions and compulsions that are driven by religious or moral thoughts. Those with a religious cultural background may experience religious obsessions and compulsions, and those without a religious affiliation may experience secular moral obsessions and compulsions. The prevalence of scrupulosity is possibly about 5 percent of those with OCD and is estimated to be higher in highly religious societies.[16]
Obsessions and Compulsions
Those with OCD generally experience both obsessions and compulsions, although some may suffer with primarily obsessional OCD (sometimes called “pure O”). In primarily obsessional OCD, the obsessions are the dominant symptom, while compulsions or rituals are present but are simply less obvious.[17] As the compulsions seen in scrupulosity are often less overt than those seen in other forms of OCD, it is common for one’s scrupulosity to be primarily obsessional.
Obsessions
Obsessions are “persistent unwanted thoughts, doubts, or images that seem intrusive, inappropriate, senseless, disturbing, and distressing.”[18] They “have no base at all in genuine desire.”[19] They are not rational. The thoughts are ego dystonic—you don’t want them, they make you feel uncomfortable, they feel threatening, and you want to resist them (but often can’t).[20] It is common for my clients to become quite enthralled with these thoughts, wanting to know what deep significance the obsession really holds for them. One Jewish woman spoke of her obsessions in this manner: “I know God doesn’t take notice of it; I know he knows it’s just an obsession, He just laughs at it, but I can’t.”[21]
There are two types of obsessions. (1) Autogenous obsessions are internally created. These are spontaneous intrusive thoughts. Examples include immoral blasphemous, sexual, or aggressive thoughts. (2) Reactive obsessions are triggered by external stimuli. Examples include contact with contamination, making a mistake, hearing religious content, or encountering asymmetry or disarray.[22] Obsessions tend to fall into several broad categories: responsibility for harm or mistakes, contamination, symmetry and order, violence and aggression, sex, and religion and morality. Obsessions tend to be most tied to the things people value most.[23]
Compulsions
Those with OCD also experience compulsions, which are deliberate, repetitive behaviors or mental acts done to try to relieve the anxiety (caused by the intrusive thoughts) and restore a feeling of safety. Compulsive behavior has a general goal of distress avoidance or minimization and includes
- an inability or unwillingness to tolerate distress;
- hasty decision making, with the goal of reducing anxiety;
- behavioral intentions to reduce anxiety or neutralize a threat;
- ego-dystonic symptoms (feelings are in conflict with or are dissonant with goals of the self);
- behavior that prevents fear of causing harm; and
- being risk averse.[24]
Compulsive rituals often have certain “rules” you must follow. They are excessive and unrealistic in their association with the fears they are seeking to diminish. They tend to fall within several broad categories: checking, decontamination, repeating actions, and ordering and arranging.[25]
Those suffering from compulsions know their behavior is self-defeating, yet they feel they can’t help themselves! Compulsions are maintained in part by negative reinforcement, which is surprisingly powerful.[26] If you have done anything that appeared to have prevented a feared and aversive outcome (e.g., taking medicine to get rid of a headache), then you are more likely to repeat it.
Those with OCD are experts at seeking reassurance. Reassurance seeking is done to quell feelings of uncertainty. One client said, “In some ways, OCD has its own addiction to assurance.” Indeed, some will go to great lengths to try to make uncertainty in their life certain—even being sneaky about it. For some it has become a destructive habit. One client commented about her husband, “He can point out when I’m seeking reassurance even when I don’t realize it.”
Reassurance-seeking people may ask questions such as, “Do you think I’ve been forgiven?,” “Am I okay?” or “Was this okay?,” “Are you sure?,” and “What if?” Or they ask the same questions repeatedly. Some may be more subtle and pose reassurance-seeking questions in a way that is not so obvious. Some seek reassurance by confessing thoughts or oversharing to get a response. Some don’t seek reassurance from another person but scour the Internet for information or opinions. Reassurance-seeking behaviors are OCD rituals.
To identify reassurance seeking, you can ask yourself, “Am I asking this question because I’m anxious?” or “Do I already know the answer?” A yes answer means it is reassurance seeking.[27] In her anxiety one client asked at the end of a therapy session, “Do you think I’ve been forgiven?” I called out the reassurance-seeking nature of the question with a bit of teasing in the lilt of my voice and reminded her that I couldn’t answer it for her, to which she added, “I know, and I know the answer.”
The International OCD Foundation has taught the difference between reassurance seeking and legitimate information seeking.[28] An information seeker asks a person a question once to be informed and accepts the answer provided. This is possible because the information seeker is asking someone who is qualified to answer the question, asking a question that is answerable, seeking the truth, asking only for the information necessary to making a decision, and accepting a relative or uncertain answer when provided. This information-seeking process contrasts with the process of seeking reassurance. A reassurance seeker asks the same question repeatedly for the purpose of lessening his or her anxiety, and often does not accept the answer given but will challenge or argue with the person asked or require the answer to be repeated, rephrased, or clarified. This occurs because the reassurance seeker is often asking anyone who will listen (often somebody not qualified to answer the question), often asking unanswerable questions, seeking a specifically desired answer, insisting on concrete, definitive answers, and will continue to seek the reassurance without making a decision or solving the problem.
Reassurance seeking falls prey to the law of diminishing returns—in time you need more and more reassurance, and yet it helps you less and less until it offers no relief whatsoever. When you last sought reassurance, how long did you feel relief before you were triggered again (if you felt any relief at all)? It may be helpful to use a coping statement when you find yourself enticed to seek reassurance. For example, “If I seek reassurance from my family and friends, even if they tell me what I hope to hear, I won’t believe them, anyway.”
Interplay of obsessions, compulsions, and reassurance seeking
To see how these elements of scrupulosity play into each other, I share here a detailed story from a person to illustrate how one moment of anxiety turned into a massive scrupulous crisis (complete with obsessions, compulsions, and multiple types of reassurance seeking). This client was a married woman in her thirties:
In my laundry room I used to keep a cup labeled “old batteries” that I would toss all our dead batteries into. I hated this cup. Battery acid made me nervous. Somewhere I read something that said batteries had to be disposed of in a special way. I didn’t know anyone else who did this, though. I even put the question out on social media once, and my aunt responded that I could actually throw them away in my kitchen trash. But I couldn’t find that in writing from someone with authority. Eventually I stopped trying to figure it out and just let the batteries pile up in the tall cup.
One day I noticed that the annoying cup was full and decided I would just recycle them that day and get it over with. I dumped them into a double bagged grocery sack and set them in the front seat of my car. I planned to recycle them at Best Buy as usual.
I went about running my errands for the day. That sack of batteries was just screaming at me to dump it, though. I needed it out of my house and out of my car. I didn’t want to have to deal with the anxiety of having to properly dispose of batteries, to be a good citizen, and make sure I was honest in all my doings.
I quickly ran into Best Buy only to find the battery recycle bins were gone. My heart sank and my anxiety spiked. I drove over to Lowe’s and ran into their store. I found their recycle bins, but my heart sank again when I saw that there was only a bin for “rechargeable” batteries. My anxiety was so high at this point. I just needed to get rid of those batteries. I walked out of the store exasperated and shoved my sack of batteries in the Lowe’s outdoor entrance trash. I got back in my car and drove to my other errands. I had already wasted so much time.
I felt better for a minute finally getting rid of the batteries, but as I was driving my anxiety started to bully me again. What if there was a rechargeable battery in my sack and I had thrown it away? I kind of remembered a white-looking battery that could have been one of those rechargeable batteries. My mother had given me some for Christmas one year. What had I done with those?
To try to ease my anxiety, I decided to look online. Maybe it wasn’t that big of a deal and I could find something that would make me feel better. Well, I made it worse! I found that rechargeable batteries really have to be recycled in a special way. In fact, in some states it was actually a law. Which states? Panic started to set in. If I broke the law, then that was a sin. I needed to get rid of this awful feeling. How would I make this right? Would I confess to a bishop? That seemed silly. Well, I definitely needed to try EVERYTHING in my power to rectify the situation. Isn’t that what the prophet would do? I decided that the only way to get rid of the feeling was to go back to the Lowe’s trash, dig out the battery sack, and then search through the entire battery bag. I needed to make sure that I was being honest and a good citizen. I needed to dispose of the batteries the right way. I needed to fix the looping in my brain.
I’m embarrassed to say that I went back to Lowe’s. But I’m filled with so much shame that I asked one of my children to come with me to just stand near me. I was too embarrassed to dig through a public trash can by myself. When I think back to this incident, the shame still stings that I involved my son in one of my OCD compulsions.
I pushed the trash can open with one hand and looked inside. I tried to move a couple of things around, but in the time I had been off running errands it must have gotten pushed down farther. I was too grossed out to go any further. I was joking and cheerful with my son trying to downplay that I accidentally threw something away that I didn’t mean to and needed it back. My anxiety subsided for a minute because I knew I had tried my best to rectify the situation. That’s all I could do, right? Had I really tried EVERYTHING, though? “Nope, not even close!” the OCD side of my brain told me. “You just need to get gloves so that you can properly dig through the trash.”
I went home, knowing that in a short time I would need to take my boys out to karate. I had been going to therapy for over a year now and had been educating myself about OCD through books. I knew these feelings were OCD, but the uncertainty and counterfeit time constraint were suffocating me. But I couldn’t let it go. In my mind, I had broken the law and committed a crime. I knew I could worry about this for the rest of my life, and it would haunt me every time I needed to get my temple recommend renewed. I talked with my husband. He tried to reassure me, but I was way past that “helping.” (I knew better than to seek for reassurance.) I was crying, angry, and embarrassed. I was so agitated. I was taking tight breaths. All of these things pointed to this situation being about OCD and not about my worthiness or about being a good citizen. I let out some of my anger by punching the couch a couple times, then went to my room.
I wanted to try to research more. I decided maybe the Internet could help ease my anxiety if I could just find the “right” article. On the contrary, I found an article that told me the state where I live is in fact one of the states with a rechargeable battery law. That sealed my fate. I kept telling myself, “This feels like OCD, so it is OCD.” I knew I was white-knuckling this whole OCD episode. I thought if I let the battery incident go, I would never be able to get rid of the guilt. I felt like I didn’t have time. The Lowe’s trash would be taken out soon and my opportunity to “fix” this would be gone. I knew this was OCD, so I tried to approach the situation with a therapy tool. I cried my way through a “thought chart.”
Despite my husband practically pleading with me to give him my gloves, trying to tell me this was just my OCD, I went back to Lowe’s and dug further in the trash and found my sack of batteries. I tried going through them in the parking lot behind my car. But that wasn’t “thorough” enough for my OCD. So, I took them home. I went in the garage because battery acid brings contamination fears and the sack had been in a public trash can during COVID times. Gross. I meticulously went through each battery to make sure it wasn’t rechargeable. There were NONE. I took the sack and put it in my regular trash can completely and totally exhausted. Shame washed over me.
I honor this client and appreciate her tremendous courage in sharing a private battle that brought so much shame and embarrassment. She is very conscientious and has had many therapy successes throughout her OCD journey, while this one was a learning experience. This painful story began with one anxious thought about battery acid, but it built into a fantastic mess as fears and obsessions about batteries, honesty, being a good citizen, and committing a crime (therefore a sin) led to compulsions and reassurance seeking both from her husband and various online sources. Have you had an experience (or perhaps many experiences) like this one?
One author’s words poignantly summarize the plight of the overly scrupulous: “OCD sets off a false fire alarm in safe circumstances. And, just like wanting to check until there is no fire, people who experience these negative morale motions just want to do the right thing to get rid of them! Typically, a series of complex compulsive behaviors is set in motion to track down what ‘wrong’ there was to make ‘right.’” [29]
Notes
[1] American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed., 189). Hereafter DSM-5.
[2] Graph of Yerkes-Dodson Law. (2007, January 5). In Wikipedia. https://
[3] Yerkes, R. M., & Dodson, J. D. (1908). The relation of strength of stimulus to rapidity of habit-formation. Journal of Comparative Neurology and Psychology, 18(5), 459–482. https://
[4] McClendon, D.T. (2019, April). Discerning your feelings: Anxiety or the Spirit? Ensign. https://
[5] Lyubomirsky,S.(2007). The how of happiness: A scientific approach to getting the life you want. Penguin Books, 181–182.
[6] Personal communication, March 8, 2016.
[7] See McClendon, D.T., McClendon, R.J.(2018). Appendix: In sickness and in health: Questions and answers relative to mental health issues and access to treatment. Commitment to the covenant: Strengthening the me, we, and thee of marriage. Religious & Studies Center, Brigham Young University, & Deseret Book.
[8] American Psychiatric Association. DSM-5, 239.
[9] Weissman, M. M., Bland, R. C., Canino, G. J., Greenwald, et al. (1994). The cross national epidemiology of obsessive compulsive disorder: The Cross National Collaborative Group. Journal of Clinical Psychiatry, 55(3, Suppl.), S5–S10.
[10] American Psychiatric Association. DSM-5, 239.
[11] Olatunji, B. O., Davis, M. L., Powers, M. B., & Smits, J. A. J. (2013). Cognitive-behavioral therapy for obsessive-compulsive disorder: A meta-analysis of treatment outcome and moderators. Journal of Psychiatric Research, 47(1), 33–41. https://
[12] Starcevic, V., Eslick, G. D., Viswasam, K., & Berle, D. (2020). Symptoms of obsessive-compulsive disorder during pregnancy and the postpartum period: A systematic review and meta-analysis. Psychiatric Quarterly, 91, 965–981.
[13] American Psychiatric Association, DSM-5, 235.
[14] American Psychiatric Association, DSM-5, 235.
[15] American Psychiatric Association. DSM-5, 237.
[16] Miller, C. H., & Hedges, D. W. (2008). Scrupulosity disorder: An overview and introductory analysis. Journal of Anxiety Disorders, 22, 1044–1046.
[17] LeJeune, C. (2023). “Pure O” OCD: Letting Go of Obsessive Thoughts with Acceptance & Commitment Therapy. New Harbinger Publications, 9, 183.
[18] Abramowitz, J. S. (2018). Getting Over OCD: A 10-step workbook for taking back your life (2nd ed.). Guilford Press, 14.
[19] Osborn, I. (2008). Can Christianity cure obsessive-compulsive disorder? A psychiatrist explores the role of faith in treatment. Brazos Press, 111.
[20] Abramowitz, 2018. Getting Over OCD, 14.
[21] Greenberg, D. (1984). Are religious compulsions religious or compulsive? A phenomenological study. American Journal of Psychotherapy, 38, 528.
[22] Shapiro, L. J. (2020). Obsessive compulsive disorder: Elements, history, treatments, and research. Praeger, 2.
[23] Abramowitz, 2018. Getting Over OCD, 15, 18.
[24] Shapiro, 2020. Obsessive compulsive disorder, 32.
[25] Abramowitz, 2018. Getting Over OCD, 20.
[26] Osborn, 2008. Can Christianity cure obsessive-compulsive disorder?, 114.
[27] Abramowitz, 2018. Getting Over OCD, 57.
[28] International OCD Foundation. 2012. The difference between reassurance-seeking and information-seeking [Seminar handout]. Anxiety Disorders Center, Saint Louis Behavioral Medicine Institute. Handout from the Behavior Therapy Training Institute at Pasadena, California, January 27–29, 2012.
[29] Shapiro, L. J. (2015). Understanding OCD: Skills to control the conscience and outsmart obsessive compulsive disorder. Praeger, 5; emphasis added.
