Health Practices and Mortality among Active California Mormons, 1980–93
James E. Enstrom
James E. Enstrom, “Health Practices and Mortality among Active California Mormons,” in Latter-day Saint Social Life: Social Research on the LDS Church and its Members (Provo, UT: Religious Studies Center, Brigham Young University, 1998), 461–472.
James E. Enstrom is research professor in the school of public health at the University of California at Los Angeles. This article is published here for the first time.
Abstract
Previous research has shown that religiously active Mormons in California are an unusually low-risk population. This study confirms and expands these findings over a much longer follow-up period. A total of 9,844 Mormon high priests and wives aged 25 years and above completed a 1979 life-style questionnaire survey, and they have now been followed for mortality for fourteen years (1980–93). Their standardized mortality ratios (SMRs) relative to U.S. whites have remained quite low over this entire period. The male SMR is 49 for all causes, 52 for cardiovascular diseases, and 47 for all cancer; the female SMR is 59 for all causes, 55 for cardiovascular diseases, and 66 for all cancer. For middle-aged high priests adhering to three health practices (never smoking cigarettes, regular physical activity, and proper sleep), the SMRs are 27 for all causes, 26 for cardiovascular diseases, and 33 for all cancer. The healthiest active Mormons have a life expectancy that is 8 to 11 years longer than U.S. whites as a whole. This study presents proportional hazards analyses that show the relative importance of several lifestyle variables on subsequent mortality.
Mormons, members of The Church of Jesus Christ of Latter-day .Saints, are a well-defined low-risk population within the United States who have provided new insights into risk factors of cancer and cardiovascular disease (Enstrom 1989). They are interesting from an epidemiological standpoint because their “Word of Wisdom” advises against the use of tobacco, alcohol, coffee, tea, and drugs. Also, the religion emphasizes a strong family life and education, advocates good health practices in general, and recommends a well-balanced diet.
Religiously active Mormons, specifically high priests, abstain essentially completely from tobacco, alcohol, and caffeine and are being examined here because they have a great difference from the general population in cancer and other death rates, as demonstrated in our previous studies (Enstrom 1989) and confirmed by others (Enstrom and Kanim 1983; Gardner and Lyon 1982). This detailed long-term assessment of the active Mormon lifestyle provides new information regarding the actual prevention of cancer and other diseases in a U.S. population. These results update and expand our previous eight-year follow-up results (Enstrom 1989).
Methods
The methods for this study have been previously described in detail (Enstrom 1989) and are only briefly summarized here. A four-page lifestyle questionnaire, with questions on major components of lifestyle, diet, and medical history, was prepared at UCLA. Then a one-time mailing of questionnaires was made by Church personnel to each of about 12,000 California high priest households with valid addresses on the Church’s computerized membership file as of about 1 December 1979. Responses were received at UCLA from 9,844 persons aged 25 years and above (5,231 high priests and 4,613 wives). The respondents have now been followed for vital status for fourteen years by computer matching with the California death file from 1 January 1980 through 31 December 1993, and 815 male and 386 female deaths have been identified among California residents and classified by underlying cause of death according to the International Classification of Diseases, Ninth Revision (ICD9). We estimate that no more than 2 percent of all California deaths among the cohort have been missed by matching based on our previous experience. Deaths occurring among cohort members who have moved out of California have not been included, but they would not affect the relative comparisons made in this study.
The California Department of Motor Vehicles (DMV) files have been used for verifying the vital status and current address of the high priest cohort members and for estimating the movement of high priest families out of California. In 1980 a total of 97 percent of cohort members and 99 percent of households were linked with the DMV drivers license file. This file has been updated regularly with notation made when individuals left California for another state or died. As of 1 January 1988, approximately 11 percent of cohort members had moved out of California according to the DMV, and we estimate that 20 percent had moved out by 1 January 1994.
Standardized mortality ratios (SMR) for major cancer sites, all cancer (ICD9 140–208), all cardiovascular diseases (ICD9 390–459), and all causes have been calculated for the total cohort as well as for the health practice subgroups. The total person-years at risk have been based on the person-years at risk among California residents. For each person the period at risk began 1 January 1980 and ended at date of death or 31 December 1993, whichever came first. Calculation of standardized mortality ratios has been done using a survival program developed by Monson (1974), with expected deaths based on concurrent death rates among U.S. whites (Enstrom 1989; Monson 1974).
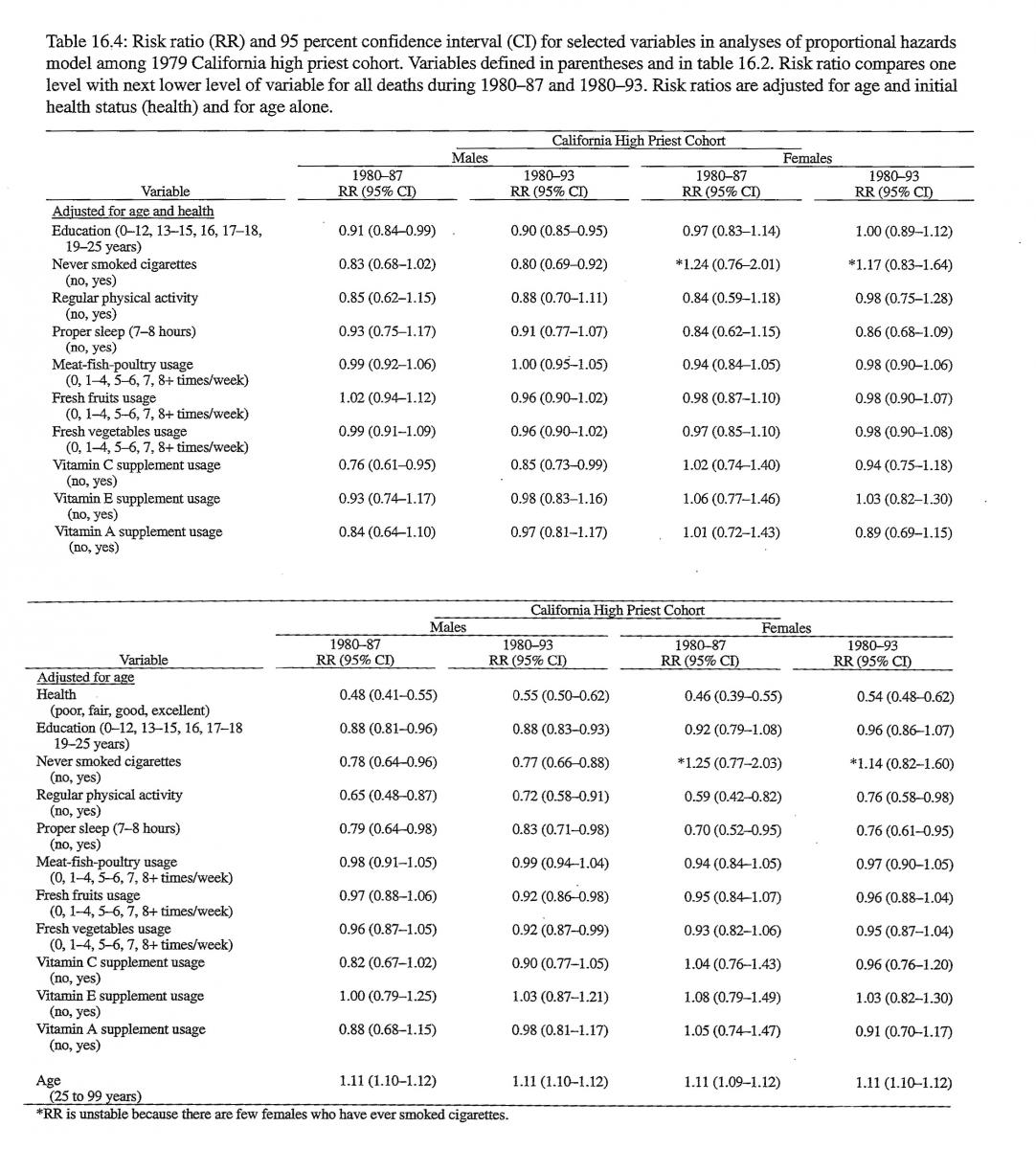
Proportional hazards linear model regression analyses have been performed for males and females for the variables of age, initial health status, education level, three health practices (never smoked cigarettes, regular physical activity, and proper sleep), consumption of meat, fish, and poultry, fresh fruits, fresh vegetables, and vitamin C, E, and A supplements. Each model includes age, initial health status, and one of the other variables (Cox and Oakes 1984). The risk ratio (RR) and 95 percent confidence interval (CI) is presented for each model for the original eight-year follow-up (1980–87) and the current fourteen-year follow-up (1980–93) (Cox and Oakes 1984).
Results
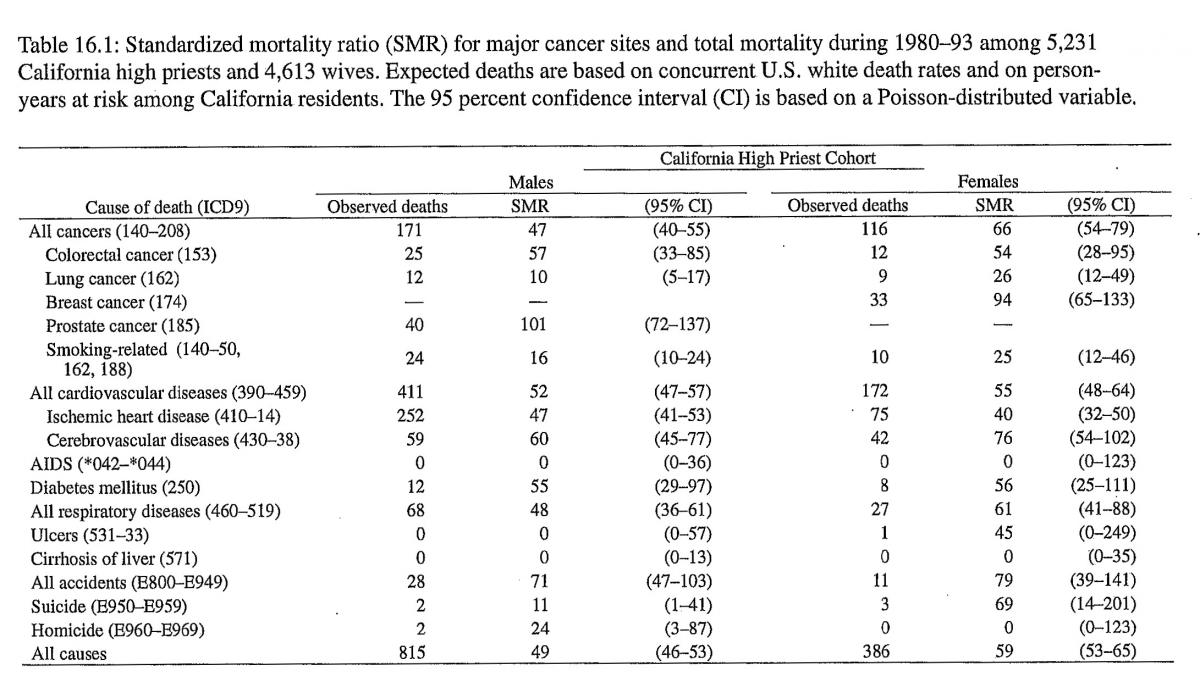
The basic demographic and health-related characteristics of the 1979 California Mormon high priest cohort are presented in our earlier paper (Enstrom 1989). The high priests generally are white, married, well educated, attend church weekly, and use essentially no tobacco, alcohol, or caffeine. Table 16.1 shows the 5,231 high priest cohort males have a 1980–93 SMR of 47 for all cancers, 16 for smoking-related cancers, 69 for cancer unrelated to smoking, and 49 for all causes, and females have somewhat similar SMRs.
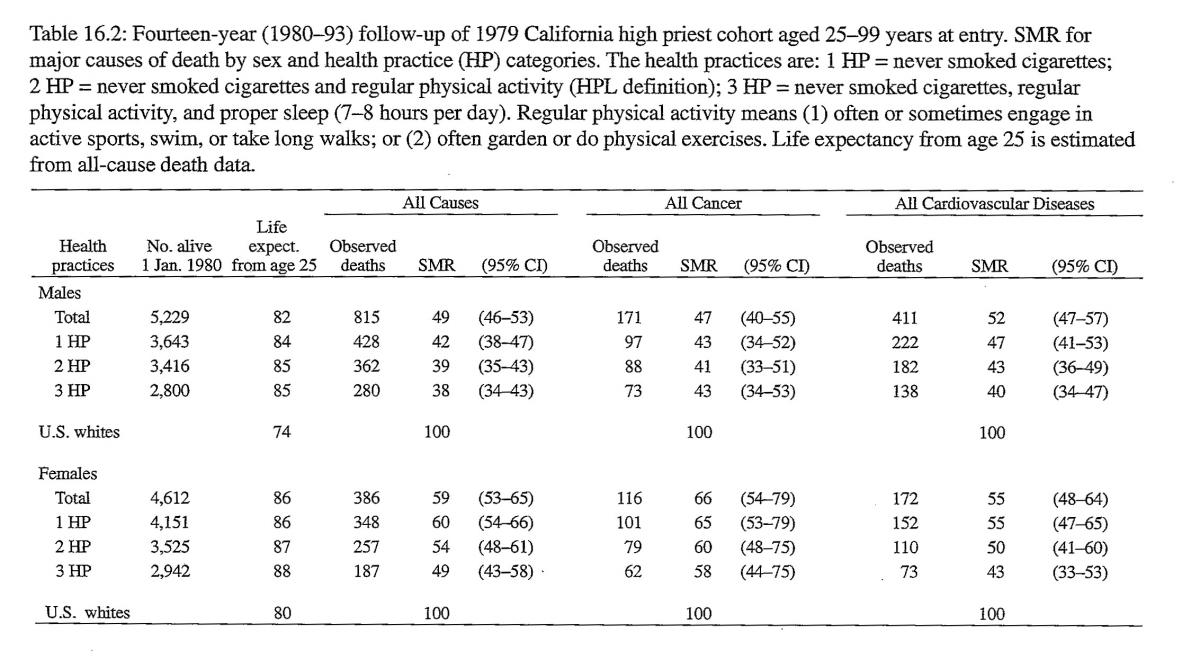
Table 16.2 shows life expectancy from age 25 and the SMRs for all causes, all cancer, and all cardiovascular diseases among the high priest cohort for all ages 25 years and above. The SMRs are presented by sex and adherence to the three health practices previously analyzed: never smoked cigarettes, regular physical activity, and proper sleep. The SMR values generally decline with increasing adherence to these practices: the all causes SMR declines from 49 to 38 for males and from 59 to 49 for females. Compared with U.S. whites, life expectancy from age 25 among those in the high priest cohort adhering to three health practices is 11 years greater for males and 8 years greater for females.
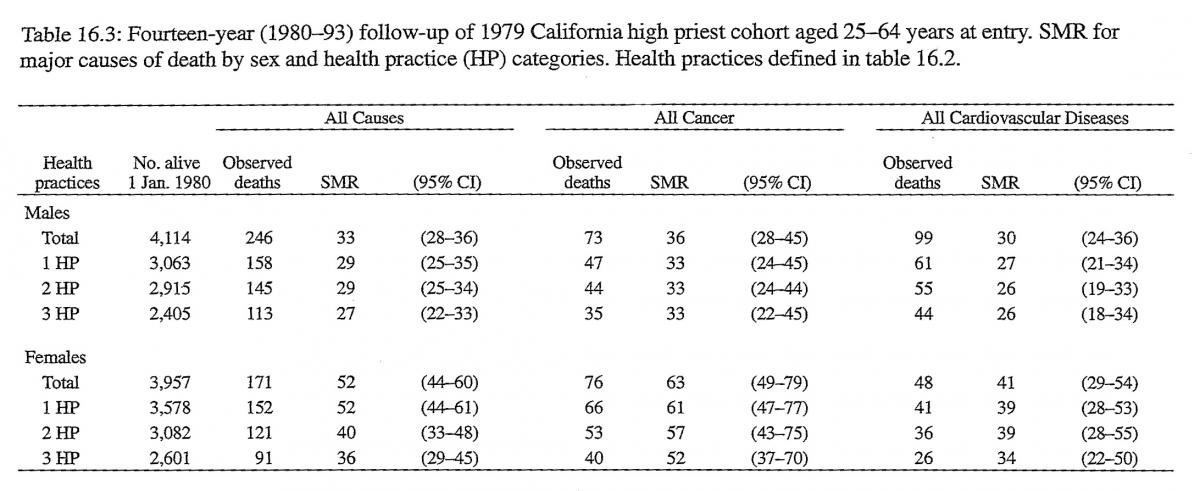
Table 16.3 shows the SMRs for all causes, all cancer, and all cardiovascular diseases for ages 25 to 64 years at entry. These SMRs are lower than the corresponding SMRs for all ages 25 years and above in table 16.2, particularly for males. Again, the SMR values decline with adherence to more health practices: the all causes SMR drops from 33 to 27 for males and from 52 to 36 for females. The declines for cancer and cardiovascular diseases are similar but not statistically significant.
Table 16.4 presents results of proportional hazards analyses for eight-year and fourteen-year follow-up and shows that age and initial health status are very strongly related to subsequent mortality. Education level and health practices and vitamin C supplement use have an inverse relationship to total mortality. The relationship is generally stronger when adjusted for age alone than when adjusted for age and initial health status. The other dietary and vitamin supplement variables show no significant relation to total mortality. These results are basically the same whether or not the models include only a few variables or all variables simultaneously. Only age and initial health status are consistently significant in all models, and they are controlled for in the risk ratios in table 16.4.
We have explored various combinations of the health and dietary practices used in the proportional hazards model, but none have yielded SMRs substantially lower than those in table 16.2. Several other health practices (proper weight for height, moderate alcohol consumption, eating breakfast, and not eating between meals), related to mortality in other studies, do not have any additional impact on the high priest cohort death rates after accounting for the three practices.
Discussion
These findings indicate that active Mormons (high priests and wives) continue to show very low cancer and total death rates that have remained fairly constant over time. These findings are supported by related research on clergy, other health conscious religious groups, social network ties, and church attendance itself (Enstrom 1989). Compared with other low-risk populations, Mormon high priests as a whole are substantially healthier than representative never smokers and similar to males in other healthy nonsmoking religious groups. High priests who never smoked cigarettes and who engage in regular physical activity have SMRs for cardiovascular diseases and all causes that are among the lowest ever reported. The reductions in cancer, cardiovascular, and total death rates are especially large in the middle age ranges. Indeed, these active Mormons are currently achieving the 50 percent reduction in cancer mortality rate that has been set as a goal for the year 2000 by the National Cancer Institute (Breslow and Cumberland 1988). Further research might reveal an even greater reduction in mortality in relationship to health practices.
Acknowledgments
This research has been supported by the American Cancer Society Grant PDT-332, National Cancer Institute Preventive Oncology Award CA 00748, and the Wallace Genetic Foundation. The author thanks the Presiding Bishopric of the LDS Church for its cooperation and thanks Linda E. Kanim and Richard J. Biermann for technical assistance.
References
Breslow, L. and W. G. Cumberland. 1988. “Progress and Objectives in Cancer Control.” Journal of the American Medical Association 259:1690–94.
Cox, D. R. and D. Oakes. 1984. Analysis of Survival Data. London: Chapman and Hall.
Enstrom, James E. 1989. “Health Practices and Cancer Mortality among Active California Mormons.” Journal of the National Cancer Institute 81:1807–14. Also in this volume.
Enstrom, James E. and Linda E. Kanim. 1983. “Populations at Low Risk.” Pp. 49–78 in Cancer Prevention in Clinical Medicine, edited by G. R. Newell. New York: Raven.
Gardner, John W. and Joseph L. Lyon. 1982. “Cancer in Utah Mormon Men by Lay Priesthood Level.” American Journal of Epidemiology 116:243–57.
Monson, R. R. 1974. “Analysis of Relative Survival and Proportional Mortality.” Comparative Biomedical Research 7:325–32.
